

Optum’s HRA gets an “F” (though employees who want more opioids will love it)
My recent request to review health risk assessments (HRAs) brought a number of responses. I’m grading the HRAs that I was able to access, on both advice and readability.
Optum’s, the second to be reviewed, receives “F” in advice and, as will be shown below, F- in readability. The scoring system is laid out here.
Advice: Chronic Pain
Optum offers the single most genius piece of advice of any of the very stable HRAs I’ve taken. By way of background, I took this HRA in 3 states where doctors are notorious for regularly giving out opioids as his or her treatment plan to follow, to people who currently have chronic pain. I checked off that I had “currently have chronic pain” just to see if they would say something worth blogging about, and was richly rewarded for that effort:

So this HRA is basically advising me to go get more opioids. The bad news is that they aren’t directing people to Quizzify’s painkiller awareness quiz. The good is that employees who want more opioids will give their program a high satisfaction rating.
Advice: Diet

This advice to switch to lowfat dairy is more likely to cause harm than to create benefit. Full-fat dairy is preferable to fat-free for most people. As this summary, with links to the studies, shows, full-fat dairy probably offers protection against diabetes.
The advice regarding “lower-fat meats” is controversial but is presented as fact. There is a whole body of research saying the opposite of what Optum says. Once again, we aren’t taking sides except to note that coercing employees to complete HRAs implies that the HRAs should be beyond challenge.
“Avoiding adding extra fats/oils when preparing food or at the table,” besides the questionable sentence structure, is simply wrong. Olive oil is on everyone’s good list, for example, while (aside from trans fats) other fats and oils have their advocates. A much better answer — how hard would it have been to come up with this? — might be “substitute olive oil for other fats and oils.” A bigger point: fats and oils make food taste good. And enjoyment of meals will lead to happier employees.
“Avoid added sugar” is decidedly unhelpful advice. Food companies go through a lot of trouble to hide “added sugar” specifically so people don’t avoid it. See this article: The Extraordinary Science of Addictive Junk Food. Optum’s go-to weapon against this cutting-edge neuroscience is: “Avoid added sugar” ?
Alas, Optum’s HRA is silent on how one goes about accomplishing this feat. This decidedly unhelpful advice runs up against the reality that people have no idea where these “added sugars” lurk, since very few products these days advertise: “An excellent source of added sugar.” By way of contrast, Quizzify does teach employees how to avoid added sugar — see the example right on the home page — and a good thing, because Quizzify’s test-takers, while improving greatly over time, originally score as follows:
- 52% think granola bars are healthy (they’re candy)
- 62% didn’t recognize synonyms for sugar (malted barley extract, dextrose, evaporated cane juice, maltodextrose)
- 68% didn’t realize that the first ingredient in a Clif Bar, organic brown rice syrup, is — you guessed it — sugar.
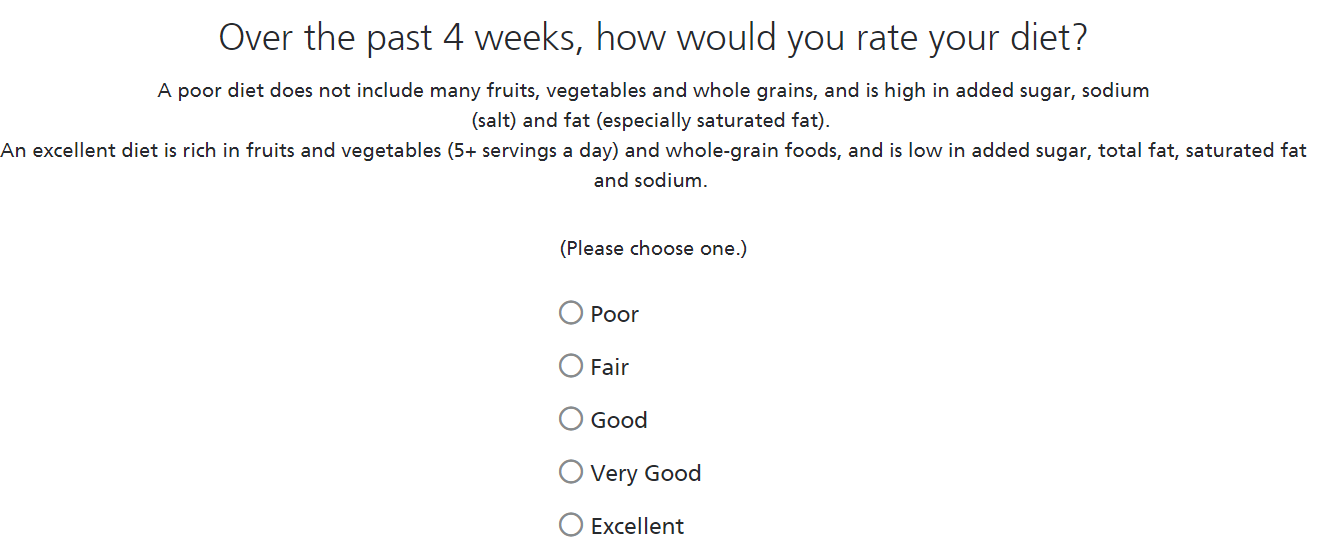
By contrast, this Optum “avoid added sugar” advice is about as helpful as just asking employees to rate their diet, which would be a useless question no HRA would ask. Oh, wait:
“An excellent diet is low in total fat” is simply wrong information. While saturated fat is controversial, the “low in total fat” myth was killed off decades ago.
While some people’s blood pressure is quite sensitive to changes in sodium intake, blanket recommendations of low-sodium diets are the subject of a great deal of controversy too. The ongoing Framingham Heart Study correlates high sodium intake with low blood pressure, the opposite of what Optum says.
So they’ve told employees to avoid fat and salt. Just to belabor the obvious — and in wellness, the obvious needs a lot of belaboring — what the bleep do they think people are going to eat instead of salty food or fats??? Are they gonna reach for kale, kelp, or a kiwi? Unlikely. They’re going to — get ready — eat something full of that very same added sugar, likely, as noted above, without even realizing it.
Congratulations, Optum. Your HRA greenlights the two biggest no-nos for employees: opioids and sugar. Fortunately for you, few employees take HRAs, seriously, so you probably aren’t doing any harm. This is especially true of yours, because even if someone did want to take yours seriously,you’ve thrown up one more roadblock: people can’t figure out what you’re saying, and that brings us to…
Readability
The complete scale for readability is here. Or so I thought, until I read Optum’s, which requires adding an “-” to the “F” on the scale . I took this HRA multiple times and each time it was an exercise in frustration.
Among other things, there were literally 100 screens that had to be scrolled through. And if you “saved” your work-in-process, you had to scroll through them all again to get back to where you left off.
Here is my favorite screen:

Stay with me on this one:
- If you are a good person, by definition, you check off the following: “I strongly agree that I am a good person.”
- If, by contrast, you are a bad person, by definition, you check off the following: “I strongly agree that I am a good person.”
After all, isn’t the whole point of being a bad person is to pretend you’re a good person? Bad people don’t exactly announce that fact on their Linkedin profiles. Sometimes they don’t even know themselves they are bad people. Walter White thinks he is a good person.

What does this mean?

Stay with me on this one.
- If you do not have asthma, meaning you are at the lowest risk, you check off the third box: “No, not being treated or taking meds.”
- If you do have asthma but are ignoring it, meaning you are at the highest risk, you check off the third box: “No, not being treated or taking meds.”
It’s also not clear how one would get treated for asthma without taking meds, making the second box a head-scratcher too.
Optum repeated this three-box choice for every other chronic disease as well, including diabetes. Diabetes, of course, is a disease that is very common to have but not be treated for. Indeed, it is so common to have diabetes and not be treated for it that there is an entire industry — that would be your industry, Optum — devoted to bribing, coaxing, cajoling or threatening every single suspected diabetic into treatment.
And yet somehow diabetes is nonetheless not common enough for you to draw an additional box on a screen that people can use to distinguish between whether they have diabetes and are not being treated for it, or whether they don’t have diabetes at all.
Indeed, one would think, with 100 screens to scroll through that could easily be consolidated into half that number (for instance, if you don’t use nicotine, you shouldn’t need to scroll through four screens to make your point), the disease inquiry category would be the wrong place to try to economize on electrons by causing people to check off the same box for opposite answers.
To summarize, I’m not following the advice on this HRA, either because it is terrible advice but I need it, or because it is great advice but I don’t need it.
Share this:

Cerner’s HRA scores an “F+”
My recent request to review health risk assessments (HRAs) brought a number of responses. I’m grading the HRAs I was able to complete, on both advice and readability.
Cerner’s, the first to be reviewed, receives “F” in advice and, as will be shown below, D in readability, for an average of F+. Advice is scored as follows:
- A: Virtually all the advice is up to date and correct
- B: The advice is generally correct
- C: There is good and bad advice in roughly equal amounts
- D: Bad advice outweighs good
- F: Employers using this HRA should caution employees not to take the advice
For each HRA being graded, unless otherwise indicated, I am completing them exactly the same way. I am somewhat understating the quality of my diet and the amount of exercise I do, in order to get “mainstream” advice.

High-risk for alcohol and drug use is incorrect. 10 mg of Ambien, taken as directed by a physician, does not create high risk in the absence of other drug and alcohol risk factors.
Ironically, there is a risk in telling people they are high-risk when they aren’t, which is that they will simply lie, in order to move their score left, out of that red segment, and out of the embarrassing range. As a result, they would not exposed to advice they should be getting if indeed they are at risk for drugs and alcohol.
And then they realize it’s OK to lie in general on HRAs. These lies take place on a massive scale, invalidating the entire HRA instrument. In an attempt to create a culture of health, companies are creating a culture of deceit.
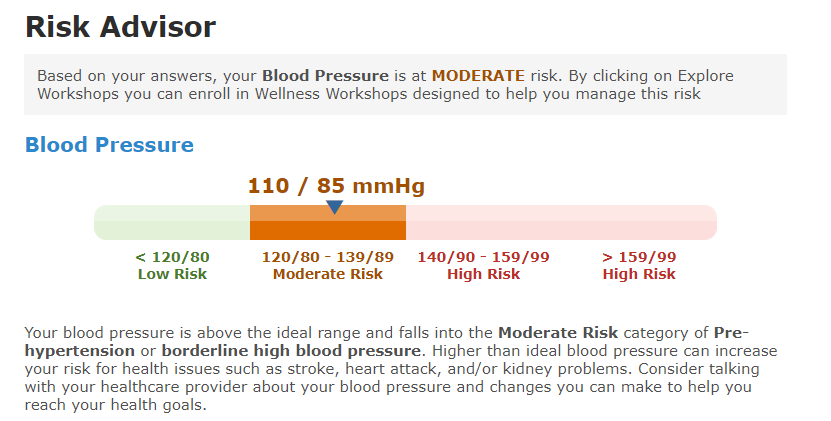
This blood pressure advice is incorrect. Someone with a “pulse pressure” of 25 (110 – 85) is not at “moderate risk” of anything. This is an emergency situation, likely indicating heart failure fluid overload. (This is not my blood pressure, by the way, or I’d be practically dead.)

This advice is wrong on five dimensions.
- People should not be taking blood pressure advice off a computer-generated algorithm, especially one that hasn’t been updated in years. That’s what doctors are for.
- It’s not at all clear that lowering sodium reduces blood pressure in the large majority of adults. This should not be offered as a fact. In some people it makes a difference. Advising people on their own situation is what doctors are for.
- “If you limit your sodium to 1500 mg a day, you can lower your blood pressure even more.” Actually the Framingham Offspring Study says the reverse. It turns out that people who say they consume 4000 mg/day of salt have the lowest blood pressure. (The link is to a lay article that itself links to scholarly material.) Not clear which is right, but advice this controversial should not be passed off as a fact when the evidence conflicts.
- It is possible that this Cerner-recommended low-sodium diet increases cardiovascular risk. Other studies, largely older ones, say this diet reduces risk. It’s safe to say there is no consensus. But HRAs, which employee are being financially coerced into doing, should not be offering controversial advice as fact.
- Telling people to avoid salty snacks may encourage people to eat sugary snacks. The HRA is quite deficient in warnings about sugar.

This advice to switch to lowfat dairy is more likely to cause harm than to create benefit. Full-fat dairy is preferable to fat-free for most people. As this summary, with links to the studies, shows, full-fat dairy probably offers protection against diabetes.
And don’t overlook their complete rookie mistake: telling employees to eat “low-fat or nonfat yogurt,” which of course is full of sugar.
The advice regarding saturated fat in meats is controversial but is presented as fact. There is a whole body of research saying the opposite of what Cerner says. Once again, we aren’t taking sides except to note that coercing employees to complete HRAs implies that the HRAs should be accurate.
Omissions
Further, Cerner’s HRA, as Yogi Berra might say, contains a lot of omissions. The following pieces of advice should be included, but aren’t:
- Advice not to text while driving (in lieu of the seat belts question*)
- Health literacy information on finding hidden sugars
- Health literacy information on finding hidden salt (who knows how much “1500 milligrams” is, assuming that advice were good?)
- Eggs are one of nature’s healthiest foods for most people
- Shingles vaccine addresses the most easily avoidable risk for people over 50
- Questions on opioid awareness (not opioid use, which people will just lie about) and information on how addictive they can be
*Not a useful question and speaks to a lack of updating. While decades ago, a few employees might have benefited from the advice to buckle a seat belt, no employee in recent history has ever not buckled their seat belt, taken an HRA on which they admitted not buckling their seat belt, read the printout that said they should buckle their seat belt, realized for the first time that not buckling a seat belt was a bad idea…and then started buckling their seat belt.
Readability
The scale for readability is:
- A: Intuitive — didn’t even think about any readability issues
- B: Readable enough
- C: Readable with exceptions
- D: Not readable in many instances
- F: Exercise in frustration
Cerner earns a “D” only because, as we will see in a future posting, it is better than Optum’s (F) and Interactive Health’s (F). Absent those two HRAs, Cerner would get an “F”.

Cerner says I am “at HIGH risk for chronic health issues.” But on the right it says I am “moderate risk.” That is confusing and decidedly unhelpful in and of itself. But wait. There’s more…now how much risk do I have?

Having sweated bullets while learning I was high risk and moderate risk, I rest easily to learn that I am at “LOW risk for chronic health issues.”
Eventually I guessed what meaning they were trying to convey, but the typical employee (who, according to Cerner, has to be told to buckle a seat belt) is not going to figure this out.
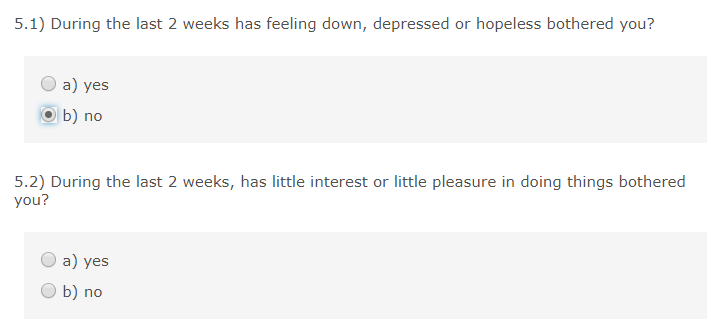
Why couldn’t they just ask if you are feeling down or depressed? (Not that any employee is going to answer that honestly, in any event.)
“Has little interest or little pleasure in doing things bothered you?” Does this mean that if having “little interest or little pleasure in doing things” doesn’t bother you, you write “no”? I had to read this several times to figure out what they were asking.
It doesn’t help that Cerner’s writing style uses a lettering system for no reason. What do those “a’s” and “b’s” add? They do that everywhere, to add to the general confusion:

Lots of extra letters, for no reason at all. And “stroke” and “heart attack” are not “conditions.” They are “events.” Heart failure (a serious disease with an average life expectancy of 5 years) should not be lumped in with angina, which can be controlled for many years with diet, exercise and medication.
Summary
There is far too much advice in here – salt, dairy, meat, drugs, blood pressure just for starters – for anyone to internalize and act upon. It is a tenet of human behavior that the more advice is given, the less is taken. Plus, more importantly, a large chunk of the advice is at least arguably wrong, if not definitely wrong.
Further, the two things that are most important for employees to learn about — sugar and opioids — are pretty much ignored. A good HRA will laser-focus on sugar harms. Likewise, opioids, the leading killer of people under 50. While an HRA can’t cure an addict, questions like: “How long does it take for the first signs of opioid addiction to start, when used as directed?” could measure people’s opioid awareness and then provide easily digestible information on what the actual answer is (3 days). Quizzify has placed its pain management-and-opioids quiz in the public domain, which could fill that gap.
The graphics with all the HIGH and LOW risk scores are very confusing.
Virtually everyone with a drinking problem will lie about it. (Just check the national statistics against the results of this HRA.) This will encourage dishonesty in other answers, and in general create the culture that it is OK to lie to one’s employer.
This HRA, and HRAs in general, make the mistake of giving the same advice to everyone who answers a certain question(s) the same way.
This health risk assessment will not provide a net benefit to a population. It is recommended not to use it, or at a very minimum insist that whoever uses it double-check any advice offered with Quizzify or another source that is up to date and accurate.
Share this:

For a good laugh, send in your vendor’s HRA for review and grading
For some reason in the last few months I’ve been deluged with requests to review health risk assessments (HRAs). Optum and Cerner top the list with multiple requests for review, while Wellsource, Redbrick, Healthmine and of course Interactive Health are also represented. Virgin Pulse too, but since it was only once and since it was with an NDA, I can’t review it except to say that any company that wants a leg up in its own marketplace should urge its closest competitors to use Virgin Pulse and insist that their employees take all the advice.
Among these HRAs, one stands out as worthwhile…and as we get into the reviews over the next month, you’ll see which one. The others shouldn’t be used, or perhaps, since for some reason employers refuse to stop using them, they carry a warning label advising employees to ignore most of the advice. The good news is that, even absent a warning label, most employees are possessed of enough common sense not to take advice from HRAs.
In other cases the advice would be straightforward and correct, like telling heavy drinkers to “cut down on your drinking,” except that virtually no heavy drinker actually admits it on an HRA. (And that particular advice, repeatedly many different ways, is about as useful as telling a depressed person to cheer up.)
You may recall that Wellsteps–the self-proclaimed “best” (meaning “worst”) program in the industry, reported only 20% of employees as drinking (meaning “70%,” the US average), and none to excess (meaning “10%,” the US average).
The self-reported smoking rate? 3%…and most smokers only smoke 3-4 days a week. How silly is that! Everyone knows smokers smoke 5 days a week, with time off for weekends, major holidays, and Beethoven’s Birthday.

In the Soviet Union, workers had a saying: “We pretend to work. They pretend to pay us.” In HRAs, it’s: “We pretend to tell the truth. They pretend to believe us.”
Your mission, should you choose to accept it
If you are an HRA user, you can have your vendor’s HRA reviewed just by giving me a username (maybe your username — you can always go in and change the answers back later if you like) and password.
If you are a vendor and want your HRA reviewed with an eye towards improving it, I can review it privately for a fee. We would then both agree whether the review can be placed publicly. You would also have the opportunity to say publicly what improvements you are planning on, based on the review.
What would be an example of a question that truly epitomizes what an HRA is all about, that will put a smile on our face?
Well, since you asked…
Um, who isn’t going to say they are a good person? Think this over a bit harder than Optum did before they decided to highlight this question as an example of their very stable geniusness:
- If you are a good person, then by definition, you will answer that you are a good person
- If you are not a good person, then by definition, you will answer that you are a good person
Example: Walter White thinks he’s a good person.

Even outcomes-based wellness vendors think they are good people, though not so good that they are willing to have me review their offerings. That’s why it’s up to you.
Share this:

Candidate running against forced wellness programs…WINS!
Paul Kramschuster, as mentioned last month on this website, launched a single-issue campaign for school board in Kansas City. Needless to say, that issue was: wellness. Blue Cross of Kansas City, CBIZ and Healthmine all had their hands in this cookie jar, at the expense of taxpayers and teachers.
He took them on…and won, becoming the second candidate (out of two in total) to win an election on a single-issue anti-“pry, poke and prod” platform.
In this hyperpartisan political environment, isn’t it reassuring that there is an issue that can unite both liberals and conservatives?
Share this:


A look back on the 5 years since Cracking Health Costs

Five years ago this month Tom Emerick and I sent out our first advance copies of Cracking Health Costs, never guessing that the book would itself “crack” the 10,000-copy plateau despite Wiley’s insistence on pricing it to make themselves a profit rather than for us to sell lots of copies. (Though if you haven’t got a copy yet, there is good news: Amazon now says “you can save an extra $2.18 at checkout.”)
Cracking attacked much of the industry power structure, way before it was fashionable to do so. (Today, of course, thanks to Dave Chase and a host of others that I dare not name due to the risk of leaving someone out, attacking the power structure has itself become a thing.) As a result, the book wasn’t terribly popular in many quarters. The Wellness Ignorati, for example, want nothing to do with it. Cracking, by the way, was the book that coined the term “Wellness Ignorati,” to describe wellness vendors and consultants who chose to ignore the fact that none of their numbers add up. Not in 2013, not now, not ever.
Some have said to call someone a member of the Wellness Ignorati was an insult. But it’s actually quite the compliment. With the exception of Wellsteps’ Steve Aldana, who has finally learned to shut up – and HERO’s Ron Goetzel and Paul Terry, who for some reason thought they could circulate a poison-pen letter to the media and not have it end up in my hands – these people have figured out that the only way to win a news cycle with us is not to participate in one.
Otherwise, here is the litany of what happens when they do create one.
A good way to see how the book has aged is to dissect the most critical review it received on Amazon, to see how it held up. This review was written by Keith McNeil, whom I have subsequently met online. He obviously put a lot of thought into it, and it deserves an equally thoughtful response. And he does have good points. (Keith, if you’re reading this, the good points come later…)
Oh, yeah—and he managed to accomplish something that none of the very stable geniuses at HERO have ever done, which is catch me with my finger on the scale.
Customer Review
By Keith McNeil on October 3, 2013
Format: Hardcover |Verified Purchase
This book has some valuable information, worthy of the two stars that I give it, but I believe it has flaws that are structural and not incidental. In the world of workplace wellness, Al Lewis and Tom Emerick (along with Vik Khanna) have created somewhat of a cottage industry by being contrarians and iconoclasts.
As is often the case with “contrarians and iconoclasts,” we are now the majority view in most of the sentiments in that book. (Not that it matters whether we are the majority, since math is not a popularity contest.)
There is nothing wrong with that to the extent that they are right and consistent in their approach, but I don’t believe that is always the case. As a matter of style, I think the book is diminished by its apparent attitude that while most of the consulting, brokerage, and wellness industry is driven by know-nothing, commission-grabbing individuals who think only of themselves and not the client, Emerick and Lewis are to be considered unbiased and pure as the wind-driven snow– while they actively sell their books and promote their consulting practices, speaking engagements, etc.
Yep, this is the case. Many wellness vendors are lying – just plug the name of your vendor into the “search” box. PBMs were another target of the book…and one just recently had to disclose in court that they were taking money under the table. Patient-centered medical homes turned out to be a scam as well.
And in terms of our being “unbiased and pure as the wind-driven snow…” We are indeed biased – biased in favor of what works. We ask everyone, if you think we are wrong in our bias, point it out. Tom and I between us have maybe 500,000 words in print at this point. However, there is an exception below—that Mr. McNeil insightfully called us out on. He was the only one to catch it.
I give it at least two stars because I think their books (which includes the book by Al Lewis, Why Nobody Believes the Numbers) do contain valuable information, as I said above, the industry is served by such contrarians who second guess the assumptions and numbers often given out (some of which they show are clearly wrong).
(Blushing) Thank you.
Nonetheless I have found a different book–by John Torinus, Jr., “The Company that Solved Health Care”–more valuable for most employers below the Fortune 1000 level and more filled with valuable ideas on how to get employees engaged and bend the cost curve. (For the record, I have no financial interest in that book and have no personal or business connection with its author.)
It turned out that Mr. Torinus “solved” healthcare by shifting a large chunk of the cost to his employees. He claimed large reductions through wellness, but when I asked him, in a conference, what reduction he got in actual wellness-sensitive medical events to support that claim. He replied that he didn’t know, but that his company’s annual death rate was “only 3%.”
“3%?” I asked. “What does your company make? Asbestos?” He immediately lost all credibility with everyone in the room. The actual death rate in the workplace is not 30 per 1000, but rather 30 per 1,000,000. In wellness, though, as I’ve subsequently observed, mistakes of three orders of magnitude are quite common. This was just the first such mistake I had ever heard.
As a broadbrush review, the Emerick|Lewis book can generally be categorized as one that believes the traditional wellness programs, health risk assessments, and biometric screenings are at best generally worthless and at worst actually harm people.
Yep. At least for outcomes-based programs. Participation-based programs don’t encourage cheating, so they are likely harmless. And if done according to guidelines, beneficial albeit unprofitable.
After beating up on most of the industry, Emerick then tries to come up with initiatives and programs that do in fact work. One of them, using Centers of Excellence, is hardly new, but Emerick tweaks it by using the term “Company-Sponsored Centers of Excellence.” (I presume that Emerick did a fine job of selecting his network and went well beyond just going with whatever organizations called themselves a Center of Excellence, which he points out can be quite deceiving.)
Yep. Tom was way ahead of his time on this one. It is fairly common among very large companies to direct employees. Walmart, for example, now considers claims for certain procedures to be out of network if they are not done at a “company-sponsored center of excellence.”
Then, after trashing most wellness plans, he heavily promotes what they consider to be wellness that works, which focuses on the employee’s “well-being.” In so doing Emerick touts, for example, the wellness vendor Healthways in its efforts along those lines. He cites studies that correlate the perception of an employee’s well-being to actual healthcare costs, with a higher sense of well-being leading to lower healthcare costs. Other than a reference to having a beautiful cafeteria and cleaning the bathrooms, the advice on how to actually increase the perceived well-being of the employees is conspicuously absent.
Mr. McNeil is completely right about this. It was a correlation, not causation, and Healthways never delivered any evidence of causation. To be perfectly honest – and at the risk of admitting that we were not “pure as the wind-driven snow”– Healthways did offer to buy a large number of books in advance if we added this chapter. The information in the chapter is correct (we can’t be “bought” to lie), but it is correlation, not causation.
He is also spot-on about our not having any “What should you do instead?” advice to “actually increase the perceived well-being of the employees.” It took another couple of years before the Quizzify lightbulb went off in my head. (Tom did indeed segue into medical travel, and is now CEO of Edison Health.)
The authors pillory most wellness vendors when, after performing their own analysis, they conclude the cost for those programs will not be returned in plan savings; but nowhere do they discuss the obvious issue of the cost to increase employee well-being. For that, their analytical skills suddenly are either turned off, or in the case of Lincoln Industries, one of the book’s real well-being success stories, the book is egregiously awry. (Emerick in the book gave fantastic well-being success rates for Lincoln Industries, but added that “resident outcomes expert Al” had not yet reviewed their findings–but he had. The Emerick book was written in early 2013, as is clear by its 2013 cited sources, but in mid-2012 Lewis posted on the Web an attack on the supposed wellness gains at Lincoln Industries–note, he made no reference to “well-being” at Lincoln Industries–and said instead of having great savings they in fact really gained nothing according to his analysis. So how did Lincoln Industries end up as a wild well-being success story in the book?)
Touche! Mr. McNeil is completely right about this too. Here is the back story. Lincoln’s information was obviously wrong, and I presented it on my previous website as such, as Mr. McNeil notes. I then got a cease-and-desist letter from them, so I took it down. That’s when I had the insight that the way that the way to “attack” people who make up numbers is with satire (which the Wellness Ignorati refer to as “sarcasm – in addition to lacking access to the internet they apparently lack access to a dictionary). Since then, I haven’t been able to beg a lawsuit out of anyone in the industry.
Share this:

AARP v. EEOC update: March 30 “progress report” issued by EEOC
In December, Judge Bates’ ruling in AARP v. EEOC (all the background is here) required the first progress report on the drafting of new incentive/penalty rules to be issued in March. We predicted there wouldn’t be any progress to report, and we were right.
A more passive-aggressive response from EEOC, submitted an hour before the deadline no less, could scarcely be imagined:
[We do] not currently have plans to issue a notice of proposed rulemaking addressing incentives for participation in employee wellness programs by a particular date certain, but [we] also have not ruled out the possibility that [we] may issue such a notice in the future.
They also noted that the top two positions at the agency remain unfilled, with nominees awaiting Senate confirmation, which makes major policy-making difficult.
The EEOC also said, according to the article linked above, that they haven’t decided whether “to float a new rule or leave its regulations as they are.”
Imagine if you are Judge Bates and you’ve told the EEOC to deep-six their old regulations. Three months later the EEOC comes back and says: “Maybe we will and maybe we won’t.” Either the EEOC didn’t run this by an attorney before they sent it out, or they are deliberately trying to antagonize the judge. Either way, they aren’t doing themselves or the wellness industry any favors.
Meanwhile, the folks at Quizzify, having completed their celebration of the pending demise of punitive “wellness or else” programs, have moved onto drafting a new HRA that will be, uniquely, compatible with the new rules, but still be NCQA-accreditable. And most importantly actually not be full of nonsense, like most of the others.
An announcement should be forthcoming within a month. Ping them if you’d like the early bird price on this.
Share this:
New data shows that “outcomes-based” (health-contingent) wellness may save money
April fools!
What follows is an analysis of all hospitalizations in the US from 2001 to 2014. Wellness–punitive, health-contingent wellness in particular–has apparently harmed more employees than it has benefited. Here’s the story in one simple graph, comparing the percentage of the hospital admissions that are wellness-sensitive (diabetes, heart attacks) to all hospital admissions. The blue line reflects that calculation for admissions covered by private (commercial) insurance, while the orange line combines Medicaid, Medicare and uninsured. They will have higher absolute rates of these events but it’s the difference of differences that matters:

What can we learn from this analysis?
- The point-to-point change is -.3% in the non-exposed population (orange) vs. +.1% in the exposed population (blue).
- The difference of differences should be going in the opposite direction, since essentially every known major factor that could impact this blue line more than the orange line is held constant, other than an increasing penetration of workplace wellness into the blue-line population. Spending about $6 billion more on wellness services in 2014 (vs. 2001) should have made a huge favorable impact on the blue line, given that the total spent on inpatient wellness-sensitive medical events in 2014 was roughly $7 billion, applying the Health Enhancement Research Organization’s estimate of $25,000/admission to the 285,000 relevant 2014 admissions.
- It’s actually worse. Only about half the employed population has access to screening and risk assessments, meaning that the size of the industry overwhelms the size of the addressable events even if one assumes that all the diagnoses leading to the events were found in screenings.
- It might seem absurd to assert that the wellness industry in total (almost $8 billion today) is double the size of the healthcare spending it is supposed to address, but a “bottoms-up” analysis gives the same answer: In the privately insured population, 4.1% of admissions were wellness-sensitive in 2014. Figure half these events take place in people who already know they are at risk or have the diagnosis. So 2% of all admissions involved employees who did not know they had the diagnosis when they had the event — and hence could conceivably have learned about it and avoided it through a wellness program. Admissions are about half of all costs, meaning 2% of admissions would consume 1% of costs. 1% of a typical $6000/individual employee spend is $60/employee/year. A wellness program, including the screening, likely costs $150. That means even a perfect program — one that finds every employee with a hidden diagnosis, avoids all false positives, and prevents every event without any added cost of prevention therapy– would lose money. Alas, as lovingly documented on this website through the years, a beam of light leaving “perfect” wouldn’t reach the “pry, poke and prod” industry for several seconds.
- The fairly dramatic upswing starting in events in the exposed population (the blue line) starting in 2012, even as the rest of the country was almost leveling off, correlates quite closely with the move towards health-contingent, or “outcomes-based” wellness, in which employees who don’t crash-diet hard enough before the final weigh-in get fined. So while a study by Redbrick showed no benefit to health-contingent programs, the truth is likely worse: many health-contingent programs actually do harm, as Interactive Health recently demonstrated and for which Wellsteps won a “best-in-industry” award. Much is this harm is visited upon employees with eating disorders.
In case you don’t believe punitive wellness programs could be this bad…
You can ask me for the raw data, and/or replicate this exact analysis, using ingredients you already have in your kitchen — an internet connection (which perhaps even Bravo has acquired by now) and the links below.
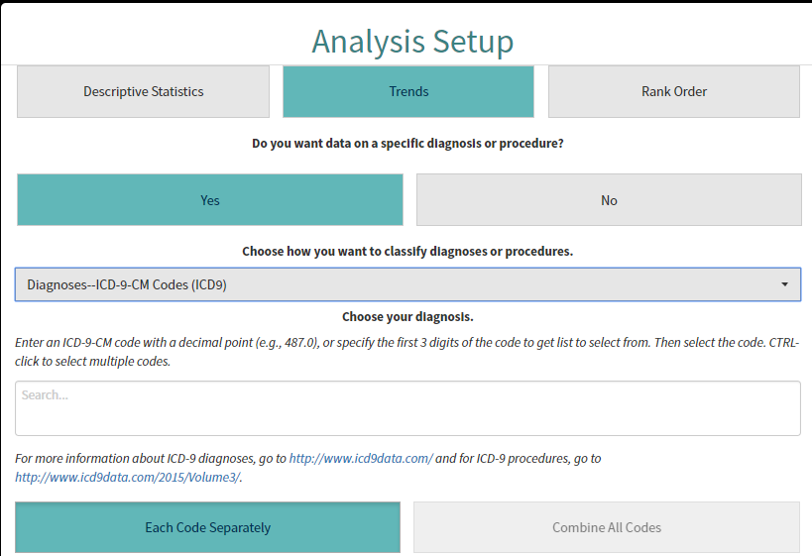
It happens that the nation’s hospital admissions data (through 2014) is all publicly available online. You can see for yourself how badly wellness has failed. First, go to the admissions database. Then under “Analysis setup” go “Trend>yes>yes.” That will bring you to a dropdown menu asking you to “choose how you want to classify the diagnoses or procedures.” Pick “Diagnosis ICD-9-CM codes.”
It will ask you to “Choose your diagnosis.” This is where it gets slightly labor-intensive. You’re gonna want to pick all the heart attack and uncomplicated diabetes codes, since those two categories represent by far the lion’s share of wellness-sensitive medical events (WSMEs), events that can be theoretically avoided through screening the stuffing out of employees. You might ask: “Why not include complications of diabetes, and heart failure etc.? Why just these two?”
That’s because we aren’t testing disease management. We’re testing to see if “playing doctor” to try to hunt for disease is worthwhile. Anyone with complications of diabetes, or a more serious condition like heart failure or COPD, obviously already knows they have it. No screen needed. We also can’t test stroke because the HCUP data prior to 2012 has some squirelliness in it. (In any event, there are far fewer strokes in the working age population than heart attacks, especially if one excludes those where atrial fibrillation was the likely cause.)
Diabetes and heart attack ICD9s begin with 250 and 410 respectively. Once you enter one of those 3-digit codes into the field, a ton of 5-digit codes will show up. Just keep hitting “CTRL click” until they all show up in the field. Then, hit “combine all codes.” Here is what the screen will look like before you do that:
After you enter these diagnoses, choose “Combine all codes” and then “Create analysis.” You’ll get a screen that looks like this. Do not attempt to adjust your TV set. I am just showing you this so you know you’re in the right place, not to try to see the results:

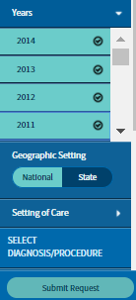
Once you’ve gotten to this point, you need to split the analysis into payer category and then pick multiple years, to show a trend. To find the payer, use the left-hand navigation bar and go to Patient Characteristics>Payer. You’ll want to do multiple years, and farther down that toolbar you’ll see “years.” You just check all the years from 2014 back to 2001 and hit “submit.” (There is some squirreliness in the years before 2001.)
Doing this by payer is critical. Almost every employee with access to workplace wellness will be commercially insured — or as HCUP puts it, privately insured.
You’ll then get a screen that looks like this:
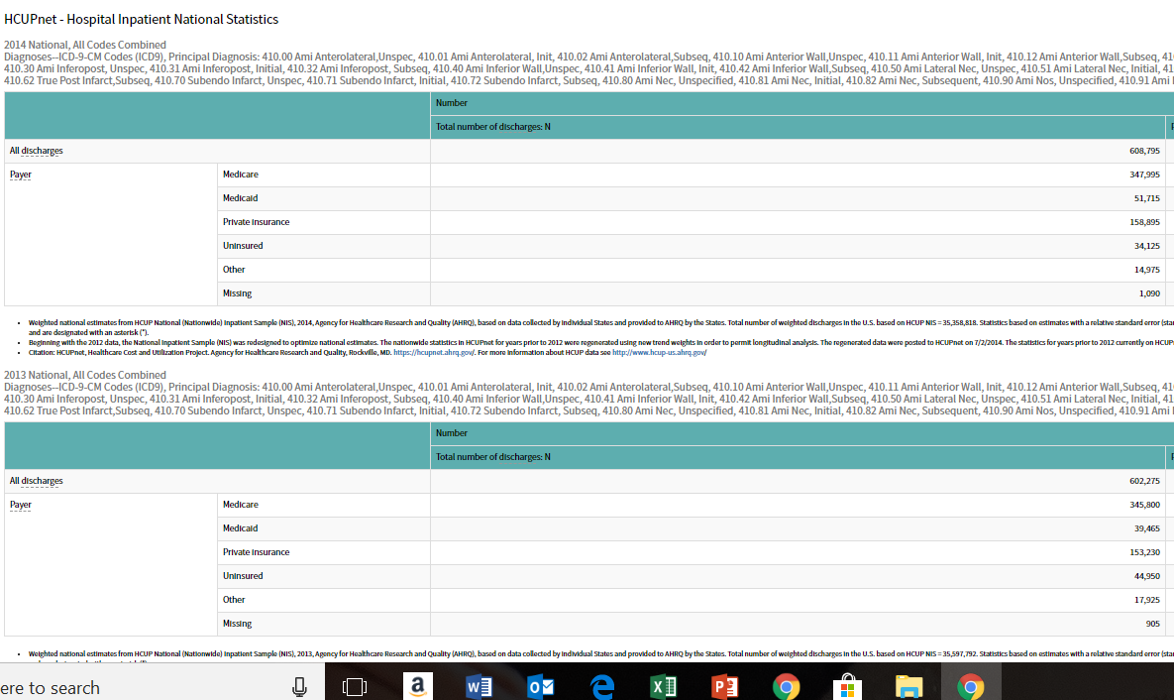
It will give you all the admissions, by payer, for all the years. You are then given an option to drop this into Excel, an option you should take. (This is the definition of “voluntary,” by the way. Your employer won’t fine you if you don’t.) Once it is in Excel, you can copy-and-paste the actual year-by-year data into an easy-to-use format, like this little snippet that lists stroke-hypertension and then repeats the format for all admissions:”All admissions” becomes the denominator for those 15 years, split into “private insurance” (where over those 15 years members had gained increasing access to wellness programs) vs. the other five categories combined, which did not have wellness access.
After you complete this analysis, you will find that the reason I offered a $3 million reward to show wellness saves money is because there is no chance of anyone ever being able to claim it.

