
Home » Wellness (Page 4)
Category Archives: Wellness
Viverae wellness primes its own pump for an EEOC wellness lawsuit
Viverae
Category: Wellness
Short Summary of Company:
“Viverae gives our clients a platform for managing healthcare costs by motivating their employees to make healthy choices. Our comprehensive wellness programs address your organization’s goals to meet your employees where they are.”
Materials Being Reviewed:

Questions for Viverae:
General: What customers have actually signed up for this and are willing to admit it?
ANS: Refused to answer
Provision #2: Since your biometrics are out of compliance with USPSTF guidelines, wouldn’t a customer be risking an EEOC lawsuit by “requiring” every employee to do this against their will, subject to a large fine?
ANS: Refused to answer
Provision #4: Isn’t this the same as saying “If you sign up for two years, we’ll give you a third year maybe at a 20% discount if you do everything perfectly, but by doing so you waive your right to cancel after one or two years” ?
ANS: Refused to answer
Provision #5: Has any customer of Viverae or any other wellness vendor with 1000 or more employees completed HRAs and submitted to biometric screens at a 100% rate, as you require in Provision #2?
ANS: Refused to answer
Provision #6: How could a health plan get a positive return on this program by offering people $720 apiece, when wellness-sensitive medical events account for less than $200/person in claims spend?
ANS: Refused to answer
Speaking of Provision #6, if your very own website says savings are $500/person (I’d be curious what legitimate academic research supports that), how can you guarantee savings when the cost of the incentive alone is $720?
ANS: Refused to answer
Share this:

Did you know 100% of your employees have chronic disease? Wellsource says so!
Wellsource
Short Summary of Company:
“Wellsource pioneered the concept of computer-assisted wellness. Today, more than 30 years later, Wellsource continues to offer innovative, evidence-based health assessments and online wellness tools that improve lives and contribute to a healthy bottom line.”
Materials being reviewed:

Questions for Wellsource
How is it that 100% of the employees at this company have a chronic disease?
ANS: Refused to answer
If “cancer” were a chronic disease as you claim it is, like diabetes or heart disease or asthma, how come no one ever says: “I have lung cancer, but my doctor says we’re staying on top of it”?
ANS: Refused to answer
If “stroke” were a chronic disease as you claim it is, how come every minute you don’t get to the ER following a stroke increases the odds you’ll end up like the Kardashians? Wouldn’t “stroke” be the epitome of an acute event rather than a chronic disease?
ANS: Refused to answer
If all these people are so sick, how come the largest opportunity per employee to save money ($40,000/employee!) is to get a few more people to buckle their seatbelts 100% of the time instead of 95% of the time?
ANS: Refused to answer
Speaking of seat belts, does it increase your credibility with potential purchasers that seat belt use is expressed the wrong way (96% buckle, meaning the correct figure to enter here would be “4%,” the ones who don’t always buckle)?
ANS: Refused to answer
If a whopping 89% of your employees have high blood pressure as defined by 140/90, do you think there is a chance you made a mistake in measuring this variable?
ANS: Refused to answer
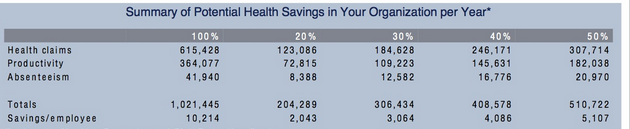
How can you save $6154.28 per employee in health spending just on these items when the average employee doesn’t spend $6154.28 in healthcare costs altogether?
ANS: Refused to answer
How is this $6154.28 savings/employee figure (expressed in your materials as $615,428 for the 100 employees in this company) consistent with sourcing Steve Aldana, who claims that you always save $1358.85 per employee, whether you get a 0% improvement or a 100% improvement in risk factors?
ANS: Refused to answer
Share this:

US Corporate Wellness Saves Money on People Who Don’t Cost Money
Category: Wellness
Short Summary of Intervention: “The strategy? Engage… Measure… Optimize. While personal accountability must always be a central component, it is supported through personal engagement and an individualized improvement process. Rather than trying to change the core of an individual employee, we work with the individual to help create a tomorrow that is a little better than today. In doing so, the organization gleans a strong ROI while simultaneously enhancing the lives of their purported ‘most important asset.’”
Materials Being Reviewed and Summary of Outcomes



Questions for US Corporate Wellness:
How can you save $350/year on people who don’t increase factors? Most people don’t add a risk factor in most years, so wouldn’t this math mean that in a couple of decades you would wipe out healthcare spending simply by doing nothing?
ANS: Refused to answer
What does “400%–The Cost of Productivity Losses to Employers Associated with Chronic Disease” mean in English? Are you saying that if no employees had chronic disease everyone would be four times as productive, meaning waiters could serve four times as many tables, doctors could see four times as many patients, pilots could fly planes four times faster, etc.?
ANS: Refused to answer
How are Denver Children’s Hospital’s wellness program participants “230% less likely to utilize the extended illness benefit” than non-participants, given that it is not possible for anyone to be 230% less likely to do anything than anyone else?
ANS: Refused to answer
Should you remove the “3.27-to-1 ROI” claim from your website now that the author of the article containing that claim has walked it back three times while the nonprofit RAND Corporation has also dismissed it and no one has ever replicated it, and the average data is from 2004?
ANS: Refused to answer
Postscript: Any apologies, explanations, changes etc. added at later dates, following the initial posting
None
Keywords: US Corporate Wellness, Brad Cooper
Share this:

Dee Edington Drains The Life Out Of The Vitality Group’s Distortion Of His Work
The Vitality Group
Short Summary of Company:
“Vitality is an active, fully integrated wellness program designed to engage your employees on their Personal Pathway to better health. Employers can choose to introduce the Vitality experience with one of our comprehensive plans. Activate is designed to bring wellness into the workplace. Elevate includes all the components of Activate, plus additional engagement features.”
Materials Being Reviewed
The Vitality Group “wearables at work” presentation. This presentation describes the health risk reduction achievable through engaging members at workplaces by wearing activity trackers.
Summary of key figures and outcomes:

Questions for Vitality Group:
You appear to be claiming that people who are “not active” reduced their risk factors simply by being engaged, without actually doing or reporting anything. A health services researcher might say that instead of taking credit for both the 6-point decline in the study group and the 5-point decline in the de facto control group risk, in reality only the difference between the two groups (1 point) could be attributable to fitness activities. If you disagree, can you explain exactly what it is that makes people in the inactive group so successful even if they don’t do anything?
ANS:
The amount that could be attributable to fitness activities is the difference between the two groups compared. For clarification, we compared (1) individuals who were engaged in fitness activities with the Vitality program (who might also be using other program elements), with (2) those who were engaged in the Vitality program on other elements but were not recording fitness activities directly with us.
So the graphic focused only on the incremental difference between the described fitness and non-fitness cohorts. Both the fitness and non-fitness cohorts were participating in other aspects of the Vitality program to track and improve their health, but the non-fitness group did not record their fitness activities through Vitality. Individuals in the non-fitness group may also have engaged in some fitness activities but simply did not log any of these activities through the Vitality program.
Observation::
Thank you for that clarification. When I look at the “difference between the two groups compared” I am seeing a 5-point decline in the first group and a 6-point decline in the second group, netting out to 1% as an “incremental difference,” rather than the 13% and 22% declines you claim,, but perhaps readers will see it differently.
How does your claim of success adjust for dropouts, and the likelihood that dropouts would have worse performance than people who were willing to be measured twice?
ANS:
This analysis did not include an adjustment for dropouts as the intent was not to make assumptions about unknown risk factors. A more detailed investigation could include this as a refinement.
Are you familiar with the concept of the “natural flow of risk” described on this slide researched and prepared by the “father of wellness measurement,” Dee Edington?
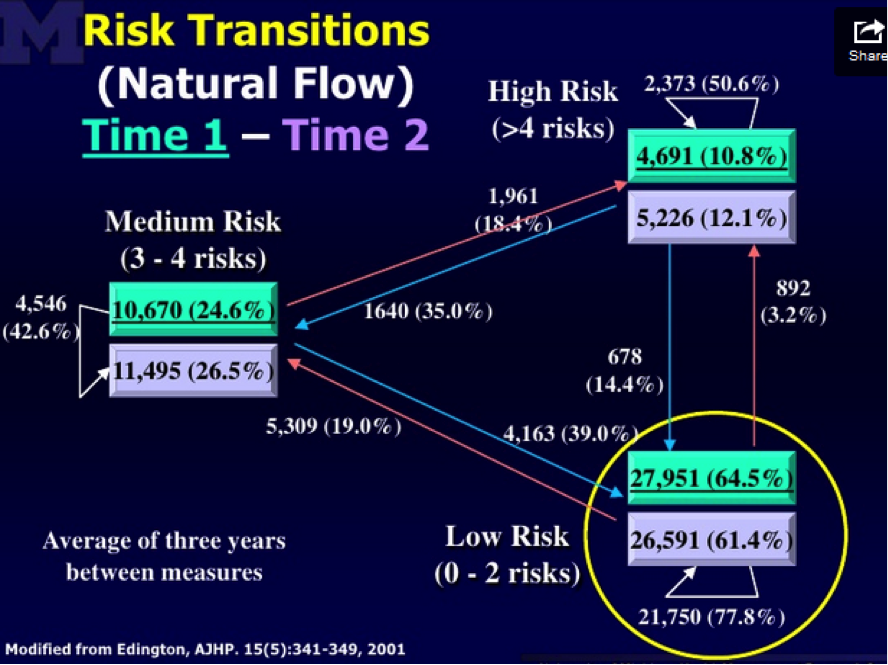
Edington’s research shows that nearly 50% of people with >4 risk factors will eventually move to a lower risk category on their own. Having been exposed to this “natural flow of risk” data, do you still believe that the non-active and active members (both groups were selected on the basis of having >4 risk factors) declined in risk due to the program, or else could some or all of the decline be due to (a) self-selection into the active group; (b) ignoring discouraged dropouts; and (c) the natural flow of risk?
Response:
Yes, we did allow for this effect by looking at the net changes in overall risk groupings by level of activity in the Vitality program. In other words, the percentages shown account for the overall flow of risk, including those who improved over the period but also those who deteriorated. The graphic focused on the proportion of high risk people in each group, but did allow for people moving into the group over the period.
Dee Edington’s work found that expected natural migration is actually a deterioration in risk groups as people naturally flow to high risk.
Often there is a tendency in wellness to compare consistent cohort risk transitions to these expected natural migration increases. Although both cohorts in the analysis saw an overall net improvement in risk groups, this comparison to natural migration was not the intent of this analysis. Instead the intent was to compare the relative changes in the two cohorts. This analysis showed that the cohort who engaged in fitness activities through Vitality had a lower proportion of high risk individuals as of their first risk measure, but had a greater net improvement in risk groups as of the last measure than those who did not engage in fitness activity through Vitality
Observation:
Hmm…well we can’t both be right. I’m looking at the exact same Dee Edington slide you are, but I am seeing the population’s risk “naturally flow” in both directions, not just “a deterioration in risk groups as people naturally flow to high risk.” Obviously the validity of the alleged declines in your cohorts is dramatically different depending on whether one uses your interpretation of Dr. Edington’s work (in which case your results are outstanding) or mine (in which case except for 1%, they are due to the natural flow downward of the highest-risk segment).
Like Alvy Singer did with Marshall McLuhan in Annie Hall, I took the liberty of asking Dee Edington himself to referee our disagreement. This is his response:
“The correct interpretation of that slide and of my work is that the natural flow of risk in a population moves in both directions, and must be understood in order to gauge impact of an intervention. It is not valid to simply start with people who were high-risk and claim credit for all risk reduction in that cohort while ignoring people who migrate in the other direction.”
Share this:

Wellnet Detects Undetected Claims Costs
Wellnet
Short Summary of Intervention:
Risk reduction program. “Our company’s focus is on exceptional execution and the manner in which health benefits are delivered and managed. Healthcare is personal and we treat it that way. Our mission to provide a level of service, collaboration and integration you will not find elsewhere in the marketplace.”
Materials Being Reviewed:

Summary of key figures and outcomes:
- 18-to-1 ROI
- $463,000 reduction ($180 per person) in medical spending, on a base of about $6 million.
- $21 million reduction in “undetected claims costs” on 55 high-risk members ($4 million) and 453 medium-risk members ($17 million).
- Medical trend reduction from 8% to 0.06%
Questions for Wellnet:
What are “undetected claims costs”? We can’t find an insurance company that has heard of them, and we can’t find any definition on Google, or even any reference to them at all, other than Wellnet’s.
ANS: Refused to answer
It’s not clear whether the 18-to-1 ROI is driven by the $180/person reduction in medical spending or the $21 million reduction in “undetected claims cost.” If the former, does that mean your wellness program only cost $10 per person?
ANS: Refused to answer
If the latter, how does the $21 million in “undetected claims costs” relate to the $6 million in detected claims costs?
ANS: Refused to answer
You list 508 medium-risk and high-risk members whose risk reduction accounted for the $21 million in “undetected claims costs.” Is it possible that many of the unmentioned 2000 employees and dependents who are low-risk might increase risk factors and therefore offset those savings, as Dee Edington’s model below would predict?
ANS: Refused to answer

By changing the axes on the graphs so that the cost bars are not drawn to scale, wouldn’t the physical difference in the height of the bars (about 50%) appear to dramatically overstate the savings (about 7.3%)? Doesn’t omitting the “$5.0” hashmark on the top graph exacerbate this effect even more?
ANS: Refused to answer
How does the 7.3% negative spending trend on the lower graph tie to the 0.06% positive spending trend claimed in the first section?
ANS: Refused to answer
On just the 55 high-risk members alone, you are saving $73,000 apiece, about 4 hospitalizations each. Can you share how this might be possible to do, through your wellness tools?
ANS: Refused to answer
Share this:

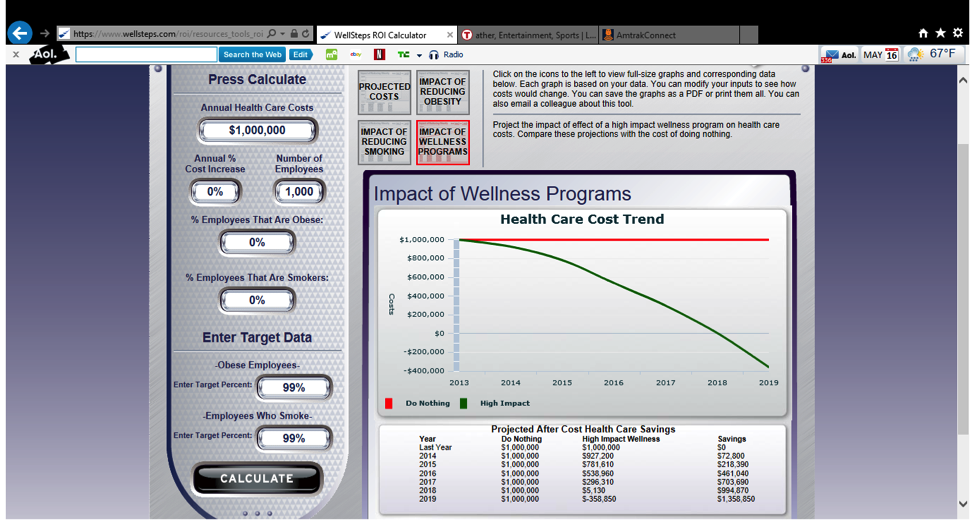
Wellsteps ROI Calculator Doesn’t Calculate ROI…and That’s the Good News
Wellsteps
Short Summary of Intervention:
“At Wellsteps, we’ve created a series of research-based ROI calculators to help you estimate the effect of well-designed wellness programs on health care costs, absenteeism, and presenteeism. Each of the three ROI calculators will examine a different employee expense and will help you determine whether investing in wellness strategies makes sense for your company. A well-designed wellness program is one that changes the health behaviors of employees, spouses, and dependents, and lowers health risks, reduces chronic disease, and helps worksites create a culture of health. The design of the WellSteps turnkey wellness solution was based partly on this body of evidence.”
Materials Being Reviewed:
Wellsteps ROI Calculator . You input your number of employees, health spending, and goals for obesity and smoking cessation. The calculator will tell you how much money you can save through the Wellsteps program.
Summary of key figures and outcomes:



Questions for Wellsteps:
In the first example above, your model calculated massive savings even with no change in obesity and smoking. In the second example, your model calculated the same massive savings even with a huge increase in obesity and smoking. It seems that no matter what smoking and obesity data we enter once we factor out inflation itself, your ROI calculator reduces healthcare costs to a level below zero by 2019. How is this possible?
ANS: Refused to answer
Shouldn’t a spike in smoking and obesity rates from 0% to 99% increase healthcare spending rather than reduce it?
ANS: Refused to answer
Your May 2014 email blast, sent out a few days after The Health Care Blog exposed your ROI model as being invalid, says your model is supported by “every wellness ROI study ever published” (a step up from being “research-based” on a “body of evidence” as your website says). We recognize that asking you to list “every wellness ROI study ever published” would be burdensome, but could you direct us to just one study that says increasing smoking and obesity can improve workforce health and/or reduce healthcare costs to below zero?
ANS: Refused to answer
Does “every wellness ROI study ever published” include the RAND studies in Health Affairs that have found negative ROIs?
ANS: Refused to answer
How are you able to “guarantee” this ROI, since it is impossible to reduce spending to a negative number?
ANS: Refused to answer
Since you’ve known that the Wellsteps ROI Calculator is invalid since this fact was pointed out to you in October 2013 and you have updated your model twice since then, how come you have elected to continue to overstate savings by a mathematically impossible figure?
ANS: Refused to answer
You lead your marketing blast by saying that “11,000 brokers and consultants” have used this ROI model? Are we the first of those 11,000 people to observe negative savings?
ANS: Refused to answer
Do you see any irony in publicly accusing one of the principals of this website, Al Lewis, of acting like a “tobacco executive lying to Congress” when even tobacco executives wouldn’t claim that smoking reduces healthcare costs like your model says it does?
ANS: Refused to answer
Where in your “ROI Calculator” can I find the ROI?
ANS: Their ROI Calculator doesn’t calculate an ROI so there was no point in even asking them to answer this question. The good news about Wellsteps is that NASA employees don’t have to worry about job security because these people are not rocket scientists.
Update: July 16, 2014
Addendum: Wellsteps accusation that I “entered false data” into the ROI calculator was posted on the “Wellness Is a Business Strategy” Linkedin Group
“It has come to our attention that an outspoken critic has entered false data into these calculators in order to make a point. We certainly support free speech; however, we wonder how valid the point can be when it is based on false data?”
“Use valid estimates for the percent of the current obese and smokers in an employee population. We provide the estimated default numbers based on national data of 33% and 20% respectively in all three calculators. In our combined 50 years of academic and consulting work, we cannot think of one employer with a 0% obesity AND 0% smoking rate. Again, valid estimates work best.”
Actually, we ran every combination of data from a reduction of 99% in smoking and obesity rates to an increase of 99% in smoking and obesity rates. Some of that data might have been “false” (whatever that means), but the result was always the same: $1358.85 in savings/employee by 2019. Here are two more examples, this time using the default numbers they recommended. The first is @$5000/employee in annual costs, with no change in smoking or obesity. The second is @50,000/employee. The answer is still the same.


How come, regardless of what assumptions get entered (and we have now entered many vastly different combinations of cost and success), the answer is always that by 2019, you save $1,358.85 per employee once you zero out inflation?
ANS: Refused to answer
Would you now admit that entering $5000/employee in spending and 33% obesity and 20% smoking (the national averages) constitute, in your words, “valid estimates that work best” ?
ANS: Refused to answer
Following my exposé, your model no longer allows a user to enter increases in smoking and obesity. Is this to prevent users from figuring out that even if the rates of smoking and obesity increase, the math underlying your model based on “every ROI study ever published” will still show a reduction of $1,358.85/employee in 2019?
ANS: Refused to answer
How come the model shows that very same $1358.85 (now finally “rounded” to $1359) potential savings from reducing obesity and smoking even if I start out with no smokers or obese employees?

Update–May 1, 2015: Wellsteps Doubles Down on Dishonesty
Two people forwarded us this, a sequel to their email that their ROI model is “based on every ROI study ever published”:
Update–September 10, 2015: Wellsteps Triples Down on Dishonesty
Somehow they reported costs going up and down at the same time. Even wellness industry math doesn’t allow that.
Share this:

ShapeUp Falls Down Trying To Do Math For Highmark
ShapeUp
“By uniting people based on common health interests and goals, and empowering them to spread the word by inviting their colleagues to join, the program created thousands of connections and enabled Highmark to build a grassroots communication strategy that reached the company’s entire employee population. This strategy, combined with the organic spread of peer-to-peer motivation, support and accountability, helps launch and sustain successful company-wide wellness challenges year after year.”
Materials Being Reviewed
ShapeUp’s Case Study of Highmark employees’ weight-loss program. Highmark is a 19,600-employee Blue Cross health plan headquartered in Pittsburgh, PA.
Summary of key figures and outcomes:


Questions for ShapeUp:
Out of Highmark’s 19,600 employees, are we right in calculating that only 163 (0.8% of the total, or 1.3% of participants) improved their BMI status?
ANS: Refused to answer
If about 9000 people (46% of 19,600) lost an average of 5.6 pounds, how come only 163 shifted to a lower weight category? Statistically speaking, shouldn’t roughly 1800 people have crossed the threshold into a lower category if the average weight loss was 5.6 pounds?
ANS: Refused to answer
Do you have a sense of how many people, on average, would improve their BMI status over this same (undisclosed) period absent a formal workplace wellness program, through initiatives undertaken on their own?
ANS: Refused to answer
How come you didn’t reveal the number of employees whose BMI status deteriorated over that period?
ANS: Refused to answer
How many people dropped out of the program, due to disappointing results or other factors?
ANS: Refused to answer
The program was quite brief, and it’s generally accepted that short-term weight loss rarely translates into long-term weight maintenance. Were participants able to keep the weight off after the program ended, or was this largely short-term weight loss?
ANS: Refused to answer
If indeed you were to add back in non-participants, dropouts, people whose BMIs went up, and people who were unable to keep the weight off after the program ended, it is possible that the 0.8% success rate would actually be lower?
ANS: Refused to answer
You equate “improved health” with reduced weight and propose “losing 10 pounds in 8 weeks,” but couldn’t reduced weight in a short period be due to crash-dieting, which would not be healthy?
ANS: Refused to answer
Why would a program as “motivating” (using your own word) as ShapeUp’s need to be accompanied by Highmark’s $4200 fines for non-participation, believed to be the highest in the country?
ANS: Refused to answer
August 20–Score one for They Said What: ShapeUp has taken down its boast about this 0.8% short-term improvement in weight classifications. We hope that this is a step in the right direction and that they will seek validation from a legitimate validation source going forward. We doubt it but look forward to being proven wrong.
March 8–Pittsburgh Post-Gazette lets Highmark pile on, explaining why they fired ShapeUp.
Share this:

Is Mercer Cooking Staywell’s Books At British Petroleum?
Staywell, Mercer
Short Summary of Intervention:
Comprehensive wellness program offered to all American employees of British Petroleum. Staywell was the vendor. Mercer was hired by British Petroleum to validate the savings claimed by Staywell.
Materials Being Reviewed
- Staywell and Mercer Analysis of British Petroleum Program
- The Health Care Blog Review of British Petroleum Wellness Program
Summary of key figures and outcomes:
No visuals were provided. A review of the articles is recommended.
Questions for Staywell and Mercer
You claimed that spending would have increased by 10.5% instead of 7% across the entire company, absent the wellness program. Since only 1139 people reduced their risk factors (not including non-participants and dropouts whose risk factors might have increased), are you saying that by reducing a risk factor, those 1139 people were responsible for the entire difference in trend for the 62,000 employees and dependents versus the original trend you projected?
ANS: Refused to answer
The savings you are claiming works out to about $17,000 for each person whose risk factors declined, almost the equivalent of avoiding one heart attack for each person who reduced a risk factor. Are you suggesting that most of those 1139 would have had heart attacks otherwise, even though fewer than 200 American BP employees had a heart attack the previous year?
Note to Staywell’s and Mercer’s actuaries: if costs decline $17,000 every time someone reduces a risk factor and your spending is about a third of that level, you can wipe out your healthcare bill by getting a third of your employees to reduce a risk factor.
ANS: Refused to answer
How does $17,000 in savings for BP employee reducing a risk factor reconcile with Staywell’s own website claiming only $100 in savings for each person reducing a risk factor in a multi-employer study?
ANS: Refused to answer
How does this unprecedented savings reconcile with the PepsiCo findings, published in a leading journal (Health Affairs) by leading researchers (RAND), that concluded applying approximately the same interventions to PepsiCo’s workforce using the same consulting firm (Mercer) actually lost money?
ANS: Refused to answer
Did Mercer notice the discrepancy between Staywell’s alleged results and PepsiCo’s (and also Staywell’s own website) and inform British Petroleum of it, since Mercer’s job was to validate this program on behalf of British Petroleum and ensure that the savings were accurate?
ANS: Refused to answer
Since a wellness program can only reduce wellness-sensitive medical events, how come you elected not to disclose the rate of wellness-sensitive medical events across the entire population before and after the program?
ANS: Refused to answer
Did you inform British Petroleum that there was an article on The Health Care Blog about their program that reached the opposite conclusion you reached?
ANS: Refused to answer
Staywell employees Jessica Grossmeier (who authored the journal article) and Paul Terry (Chief Science Officer) were asked privately and by many of the people who posted comments to rebut The Health Care Blog and declined. Wouldn’t it have been a useful discussion to explain to readers how British Petroleum could have saved more than 100 times what you yourself said was possible?
ANS: Refused to answer
Share this:

Mercer Says “Choice of Trend” Drives Savings Estimates
Mercer
Short Summary of Intervention as described by company:
Mercer Health AdvantageSM – Mercer Health Advantage (MHA) allows self-funded employers to enroll their employees in new medical plans starting January 1, 2013. These programs are designed to save employers 5% or more of medical plan cost with the same plan design they have in place today. The savings come from select networks with providers chosen for their quality and cost effectiveness. Employers also gain access to dedicated MHA clinical care management with ongoing oversight and audit by a team of Mercer clinicians. Mercer plans to offer MHA to smaller self-funded employers in 2014. Self-insured clients with Aetna need 1,000 employees, Anthem-1,500 employees or greater on WGS or NASCO claims platform and UHC must have 3,000 employees in the National Accounts segment.
Materials Being Reviewed
All publicly available Mercer outcomes reports and related materials, plus Mercer Health Advantage
Related materials:
- Georgia Medicaid
- North Carolina Outcomes Excerpts below
- Staywell and British Petroleum
Summary of key figures and outcomes:
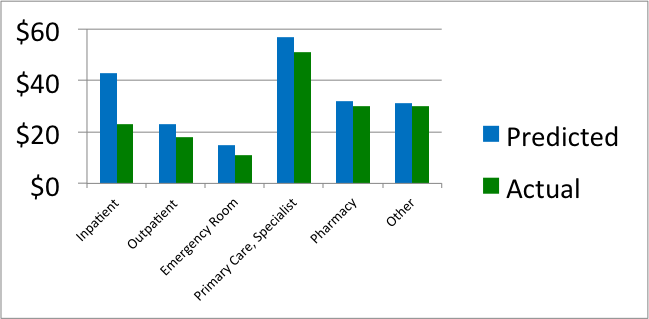
Comparison of actual vs. predicted spending per North Carolina Medicaid member per month in medical home, by category of service
Predicted vs. actual by age grouping for North Carolina Medicaid enrollees in medical home
 Questions for Mercer
Questions for Mercer
I: Mercer Health Advantage
Since most employers spend less than 5% of their total budget on disease management-sensitive events, how is it possible to save 5% through a disease management program even by eliminating every event with no increase in preventive expenses?
ANS: Refused to answer
If the state of Georgia were able to save 19% through APS disease management, which according to your own reconciliation APS is able to do, shouldn’t you be advising clients to use APS or another vendor instead of yourselves?
ANS: Refused to answer
If you are being retained to help a client find the best disease management solution, wouldn’t offering your own such solution create a conflict of interest?
ANS: Refused to answer
How have you determined the quality and cost-effectiveness of physicians that you “choose” for this network?
ANS: Refused to answer
II: Mercer North Carolina Patient-Centered Medical Home Analysis
The first North Carolina chart shows savings in every category. How is it possible to save money in all categories? Doesn’t some component of spending have to go up to make everything else come down? Or, as the outcomes measurement textbook says: “If you insulate your house, you’ll save money on heat, but not on insulation.”
ANS: Refused to answer
Is it possible that the reason savings appeared in all categories is that you simply chose to project a high trend, so that you could show more savings against that trend, or as you’ve said in the past: ““We can conclude…that the choice of trend has a large impact on estimates of financial savings”?
ANS: Refused to answer
If medical homes save money through more primary care reducing the need for specialist visits, why combine both categories when reporting savings?
ANS: Refused to answer
Inpatient spending fell by more than 50%, which implies that non-birth-event admissions would have fallen by more than 70%. How does this reconcile with the official government admissions data, which shows no change in admissions?
ANS: Refused to answer
There was no noticeable decline in North Carolina in the official government list of primary care-sensitive admissions during the period you analyzed. How do you reconcile that data with your own data showing massive admissions reduction?
ANS: Refused to answer
The second North Carolina chart shows that per-member per-month expenses in children under 1 year of age declined more than 50%. Since there is essentially no common chronic disease in this age group, where did the savings come from?
ANS: Refused to answer
The largest expenditure in this age group is in neonates. How does your data reconcile with the government data showing no change in neonatal admissions?
ANS: Refused to answer
How were you able to show such massive savings for this age group in your medical home analysis when this age group wasn’t eligible for the medical home?
ANS: Refused to answer
III: Mercer Georgia Analysis
Assuming that disease management-sensitive medical events account for roughly 8% of spending in a Medicaid population, how is it possible to save 19% through a disease management program?
ANS: Refused to answer
How do you reconcile your conclusion that the APS disease management program saved 19%, when an FBI investigation found that APS had largely failed to perform its disease management services?
ANS: Refused to answer
IV: Staywell and British Petroleum
Did you caution British Petroleum that the savings you validated for them was at least 100 times the savings that Staywell itself claims is possible?
ANS: Refused to answer
Did you question Staywell about how they were able to outperform their benchmark by 100-fold?
ANS: Refused to answer
Why didn’t you or Staywell provide your viewpoint when requested to, following the observations on The Health Care Blog that these savings were mathematically impossible?
ANS: Refused to answer
V: Mercer Qualifications to Do Outcomes Analysis
It appears that no one at Mercer has ever achieved Advanced or even Standard Certification in Critical Outcomes Report Analysis, either through DMPC or one for the Validation Institute that is specifically geared to benefits consultants. Has any Mercer consultant taken either course and failed, or has no one at Mercer ever taken either course?
ANS: Refused to answer
Assuming the mistakes highlighted above are innocent miscalculations and not purposeful deceptions – and with senior consultant hourly billing rates well in excess of $500/hour – don’t you think it would be a good idea to become qualified in analyzing outcomes reports and reconciliation methodologies that you are being paid to analyze?
ANS: Refused to answer
Is there another course in outcomes analysis that we are unaware of that your consultants have taken, and if so, how did they still make all the mistakes above?
ANS: Refused to answer
Share this:

American Heart Association promotes StayWell while violating its conflict of interest policy
American Heart Association, StayWell
Short Summary of Company:
AHA wellness: “The American Heart Association’s Worksite Wellness Kit encourages companies to give employees an excuse to get away from their desks.”
Staywell: “StayWell helps clients across the health care spectrum address the changing landscape like no other company. We leverage the latest technology, enhanced analytics, and deep consumer insights in an integrated portfolio of best-in-class client solutions.”
Materials Being Reviewed
- The Role of Worksite Health Screening: A Policy Statement
- The Health Care Blog’s Observations on that Policy
Questions for AHA
Your conflict-of-interest statement says you “make every effort to avoid actual or potential conflicts of interest that may arise as a result of an outside relationship.” Why doesn’t letting the Chief Science Officer of a wellness company write your wellness policy citing his own articles in support of wellness violate that policy?
ANS: Refused to answer
Were you aware that Staywell perpetrated a scheme in which they worked with Mercer to convince British Petroleum that their outcomes were 100 times better than what Staywell itself said was possible?
ANS: Refused to answer
Why did you allow a writer to source his own articles, thus creating an AHA policy stand that is clearly in his own financial interest?
ANS: Refused to answer
Is it representative of your peer review policy not to “vet” your peer reviewers to see if they themselves were involved in scandals that are very relevant to the article they are reviewing?
ANS: Refused to answer
Why did you as an organization and the writers of that policy decline The Health Care Blog’s invitation to defend your article against observations that it was totally conflicted and based on data known to be invalid?
ANS: Refused to answer
Why did you allow the writers to cherry-pick the available literature, ignoring the overwhelming evidence against your policy and instead continue to cite the old “Harvard study” whose lead author has now walked it back three times?
ANS: Refused to answer
Why did your editors allow the writers to call this (disavowed) Harvard study “recent” even though it was written in 2009 using data with an average date of 2004?
ANS: Refused to answer
Why did your writers knowingly cite studies that no legitimate health services researcher would find acceptable due to obvious study design flaws, like comparing active motivated participants to non-motivated non-participants, claiming that an outcome on volunteers who persisted in the program for three years is representative of the population as a whole, and taking credit for risk reductions in previously high-risk people that would have happened anyway?
ANS: Refused to answer
Why didn’t you mention that the screening frequencies you are endorsing are far in excess of guidelines set by the United States Preventive Services Task Force?
ANS: Refused to answer
As an association named for the human heart, how come you didn’t publish cautions that the screening frequencies you’re recommending can lead to overdiagnosis, overtreatment and other cardiometabolic harms?
ANS: Refused to answer
Postscript: Any apologies, retractions, explanations etc. other than answering the questions
A July 17 email from co-author Ross Arena: “I am troubled by these accusations, as is AHA. I have included an AHA representative who will address this.” [No AHA response followed.]
A July 17 response from us noted that technically these are observations, not accusations. We “observed” that their screening policy was co-authored by the CEO of a screening company. (We offered to link them to dictionary.com to see the difference between the two words, but they declined.)
