
Mercer
Short Summary of Intervention as described by company:
Mercer Health AdvantageSM – Mercer Health Advantage (MHA) allows self-funded employers to enroll their employees in new medical plans starting January 1, 2013. These programs are designed to save employers 5% or more of medical plan cost with the same plan design they have in place today. The savings come from select networks with providers chosen for their quality and cost effectiveness. Employers also gain access to dedicated MHA clinical care management with ongoing oversight and audit by a team of Mercer clinicians. Mercer plans to offer MHA to smaller self-funded employers in 2014. Self-insured clients with Aetna need 1,000 employees, Anthem-1,500 employees or greater on WGS or NASCO claims platform and UHC must have 3,000 employees in the National Accounts segment.
Materials Being Reviewed
All publicly available Mercer outcomes reports and related materials, plus Mercer Health Advantage
Related materials:
- Georgia Medicaid
- North Carolina Outcomes Excerpts below
- Staywell and British Petroleum
Summary of key figures and outcomes:
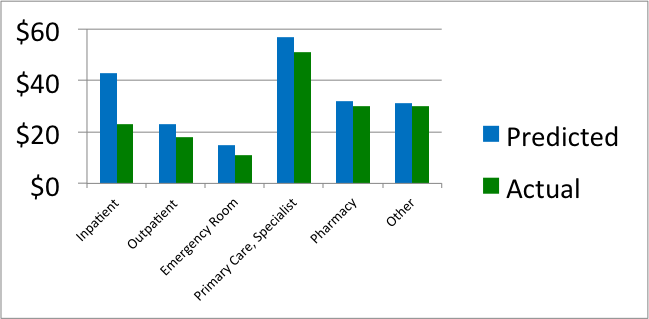
Comparison of actual vs. predicted spending per North Carolina Medicaid member per month in medical home, by category of service
Predicted vs. actual by age grouping for North Carolina Medicaid enrollees in medical home
 Questions for Mercer
Questions for Mercer
I: Mercer Health Advantage
Since most employers spend less than 5% of their total budget on disease management-sensitive events, how is it possible to save 5% through a disease management program even by eliminating every event with no increase in preventive expenses?
ANS: Refused to answer
If the state of Georgia were able to save 19% through APS disease management, which according to your own reconciliation APS is able to do, shouldn’t you be advising clients to use APS or another vendor instead of yourselves?
ANS: Refused to answer
If you are being retained to help a client find the best disease management solution, wouldn’t offering your own such solution create a conflict of interest?
ANS: Refused to answer
How have you determined the quality and cost-effectiveness of physicians that you “choose” for this network?
ANS: Refused to answer
II: Mercer North Carolina Patient-Centered Medical Home Analysis
The first North Carolina chart shows savings in every category. How is it possible to save money in all categories? Doesn’t some component of spending have to go up to make everything else come down? Or, as the outcomes measurement textbook says: “If you insulate your house, you’ll save money on heat, but not on insulation.”
ANS: Refused to answer
Is it possible that the reason savings appeared in all categories is that you simply chose to project a high trend, so that you could show more savings against that trend, or as you’ve said in the past: ““We can conclude…that the choice of trend has a large impact on estimates of financial savings”?
ANS: Refused to answer
If medical homes save money through more primary care reducing the need for specialist visits, why combine both categories when reporting savings?
ANS: Refused to answer
Inpatient spending fell by more than 50%, which implies that non-birth-event admissions would have fallen by more than 70%. How does this reconcile with the official government admissions data, which shows no change in admissions?
ANS: Refused to answer
There was no noticeable decline in North Carolina in the official government list of primary care-sensitive admissions during the period you analyzed. How do you reconcile that data with your own data showing massive admissions reduction?
ANS: Refused to answer
The second North Carolina chart shows that per-member per-month expenses in children under 1 year of age declined more than 50%. Since there is essentially no common chronic disease in this age group, where did the savings come from?
ANS: Refused to answer
The largest expenditure in this age group is in neonates. How does your data reconcile with the government data showing no change in neonatal admissions?
ANS: Refused to answer
How were you able to show such massive savings for this age group in your medical home analysis when this age group wasn’t eligible for the medical home?
ANS: Refused to answer
III: Mercer Georgia Analysis
Assuming that disease management-sensitive medical events account for roughly 8% of spending in a Medicaid population, how is it possible to save 19% through a disease management program?
ANS: Refused to answer
How do you reconcile your conclusion that the APS disease management program saved 19%, when an FBI investigation found that APS had largely failed to perform its disease management services?
ANS: Refused to answer
IV: Staywell and British Petroleum
Did you caution British Petroleum that the savings you validated for them was at least 100 times the savings that Staywell itself claims is possible?
ANS: Refused to answer
Did you question Staywell about how they were able to outperform their benchmark by 100-fold?
ANS: Refused to answer
Why didn’t you or Staywell provide your viewpoint when requested to, following the observations on The Health Care Blog that these savings were mathematically impossible?
ANS: Refused to answer
V: Mercer Qualifications to Do Outcomes Analysis
It appears that no one at Mercer has ever achieved Advanced or even Standard Certification in Critical Outcomes Report Analysis, either through DMPC or one for the Validation Institute that is specifically geared to benefits consultants. Has any Mercer consultant taken either course and failed, or has no one at Mercer ever taken either course?
ANS: Refused to answer
Assuming the mistakes highlighted above are innocent miscalculations and not purposeful deceptions – and with senior consultant hourly billing rates well in excess of $500/hour – don’t you think it would be a good idea to become qualified in analyzing outcomes reports and reconciliation methodologies that you are being paid to analyze?
ANS: Refused to answer
Is there another course in outcomes analysis that we are unaware of that your consultants have taken, and if so, how did they still make all the mistakes above?
ANS: Refused to answer

