Mercer Says “Choice of Trend” Drives Savings Estimates
Mercer
Short Summary of Intervention as described by company:
Mercer Health AdvantageSM – Mercer Health Advantage (MHA) allows self-funded employers to enroll their employees in new medical plans starting January 1, 2013. These programs are designed to save employers 5% or more of medical plan cost with the same plan design they have in place today. The savings come from select networks with providers chosen for their quality and cost effectiveness. Employers also gain access to dedicated MHA clinical care management with ongoing oversight and audit by a team of Mercer clinicians. Mercer plans to offer MHA to smaller self-funded employers in 2014. Self-insured clients with Aetna need 1,000 employees, Anthem-1,500 employees or greater on WGS or NASCO claims platform and UHC must have 3,000 employees in the National Accounts segment.
Materials Being Reviewed
All publicly available Mercer outcomes reports and related materials, plus Mercer Health Advantage
Related materials:
- Georgia Medicaid
- North Carolina Outcomes Excerpts below
- Staywell and British Petroleum
Summary of key figures and outcomes:
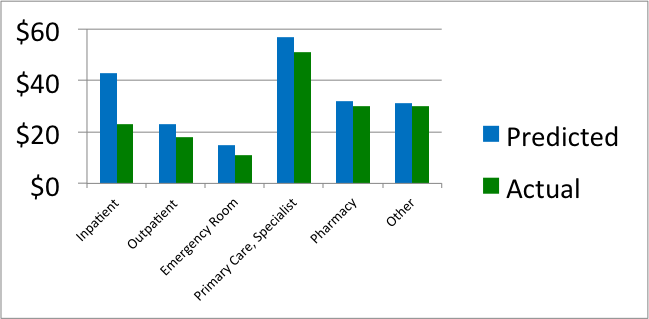
Comparison of actual vs. predicted spending per North Carolina Medicaid member per month in medical home, by category of service
Predicted vs. actual by age grouping for North Carolina Medicaid enrollees in medical home
 Questions for Mercer
Questions for Mercer
I: Mercer Health Advantage
Since most employers spend less than 5% of their total budget on disease management-sensitive events, how is it possible to save 5% through a disease management program even by eliminating every event with no increase in preventive expenses?
ANS: Refused to answer
If the state of Georgia were able to save 19% through APS disease management, which according to your own reconciliation APS is able to do, shouldn’t you be advising clients to use APS or another vendor instead of yourselves?
ANS: Refused to answer
If you are being retained to help a client find the best disease management solution, wouldn’t offering your own such solution create a conflict of interest?
ANS: Refused to answer
How have you determined the quality and cost-effectiveness of physicians that you “choose” for this network?
ANS: Refused to answer
II: Mercer North Carolina Patient-Centered Medical Home Analysis
The first North Carolina chart shows savings in every category. How is it possible to save money in all categories? Doesn’t some component of spending have to go up to make everything else come down? Or, as the outcomes measurement textbook says: “If you insulate your house, you’ll save money on heat, but not on insulation.”
ANS: Refused to answer
Is it possible that the reason savings appeared in all categories is that you simply chose to project a high trend, so that you could show more savings against that trend, or as you’ve said in the past: ““We can conclude…that the choice of trend has a large impact on estimates of financial savings”?
ANS: Refused to answer
If medical homes save money through more primary care reducing the need for specialist visits, why combine both categories when reporting savings?
ANS: Refused to answer
Inpatient spending fell by more than 50%, which implies that non-birth-event admissions would have fallen by more than 70%. How does this reconcile with the official government admissions data, which shows no change in admissions?
ANS: Refused to answer
There was no noticeable decline in North Carolina in the official government list of primary care-sensitive admissions during the period you analyzed. How do you reconcile that data with your own data showing massive admissions reduction?
ANS: Refused to answer
The second North Carolina chart shows that per-member per-month expenses in children under 1 year of age declined more than 50%. Since there is essentially no common chronic disease in this age group, where did the savings come from?
ANS: Refused to answer
The largest expenditure in this age group is in neonates. How does your data reconcile with the government data showing no change in neonatal admissions?
ANS: Refused to answer
How were you able to show such massive savings for this age group in your medical home analysis when this age group wasn’t eligible for the medical home?
ANS: Refused to answer
III: Mercer Georgia Analysis
Assuming that disease management-sensitive medical events account for roughly 8% of spending in a Medicaid population, how is it possible to save 19% through a disease management program?
ANS: Refused to answer
How do you reconcile your conclusion that the APS disease management program saved 19%, when an FBI investigation found that APS had largely failed to perform its disease management services?
ANS: Refused to answer
IV: Staywell and British Petroleum
Did you caution British Petroleum that the savings you validated for them was at least 100 times the savings that Staywell itself claims is possible?
ANS: Refused to answer
Did you question Staywell about how they were able to outperform their benchmark by 100-fold?
ANS: Refused to answer
Why didn’t you or Staywell provide your viewpoint when requested to, following the observations on The Health Care Blog that these savings were mathematically impossible?
ANS: Refused to answer
V: Mercer Qualifications to Do Outcomes Analysis
It appears that no one at Mercer has ever achieved Advanced or even Standard Certification in Critical Outcomes Report Analysis, either through DMPC or one for the Validation Institute that is specifically geared to benefits consultants. Has any Mercer consultant taken either course and failed, or has no one at Mercer ever taken either course?
ANS: Refused to answer
Assuming the mistakes highlighted above are innocent miscalculations and not purposeful deceptions – and with senior consultant hourly billing rates well in excess of $500/hour – don’t you think it would be a good idea to become qualified in analyzing outcomes reports and reconciliation methodologies that you are being paid to analyze?
ANS: Refused to answer
Is there another course in outcomes analysis that we are unaware of that your consultants have taken, and if so, how did they still make all the mistakes above?
ANS: Refused to answer
Share this:

American Heart Association promotes StayWell while violating its conflict of interest policy
American Heart Association, StayWell
Short Summary of Company:
AHA wellness: “The American Heart Association’s Worksite Wellness Kit encourages companies to give employees an excuse to get away from their desks.”
Staywell: “StayWell helps clients across the health care spectrum address the changing landscape like no other company. We leverage the latest technology, enhanced analytics, and deep consumer insights in an integrated portfolio of best-in-class client solutions.”
Materials Being Reviewed
- The Role of Worksite Health Screening: A Policy Statement
- The Health Care Blog’s Observations on that Policy
Questions for AHA
Your conflict-of-interest statement says you “make every effort to avoid actual or potential conflicts of interest that may arise as a result of an outside relationship.” Why doesn’t letting the Chief Science Officer of a wellness company write your wellness policy citing his own articles in support of wellness violate that policy?
ANS: Refused to answer
Were you aware that Staywell perpetrated a scheme in which they worked with Mercer to convince British Petroleum that their outcomes were 100 times better than what Staywell itself said was possible?
ANS: Refused to answer
Why did you allow a writer to source his own articles, thus creating an AHA policy stand that is clearly in his own financial interest?
ANS: Refused to answer
Is it representative of your peer review policy not to “vet” your peer reviewers to see if they themselves were involved in scandals that are very relevant to the article they are reviewing?
ANS: Refused to answer
Why did you as an organization and the writers of that policy decline The Health Care Blog’s invitation to defend your article against observations that it was totally conflicted and based on data known to be invalid?
ANS: Refused to answer
Why did you allow the writers to cherry-pick the available literature, ignoring the overwhelming evidence against your policy and instead continue to cite the old “Harvard study” whose lead author has now walked it back three times?
ANS: Refused to answer
Why did your editors allow the writers to call this (disavowed) Harvard study “recent” even though it was written in 2009 using data with an average date of 2004?
ANS: Refused to answer
Why did your writers knowingly cite studies that no legitimate health services researcher would find acceptable due to obvious study design flaws, like comparing active motivated participants to non-motivated non-participants, claiming that an outcome on volunteers who persisted in the program for three years is representative of the population as a whole, and taking credit for risk reductions in previously high-risk people that would have happened anyway?
ANS: Refused to answer
Why didn’t you mention that the screening frequencies you are endorsing are far in excess of guidelines set by the United States Preventive Services Task Force?
ANS: Refused to answer
As an association named for the human heart, how come you didn’t publish cautions that the screening frequencies you’re recommending can lead to overdiagnosis, overtreatment and other cardiometabolic harms?
ANS: Refused to answer
Postscript: Any apologies, retractions, explanations etc. other than answering the questions
A July 17 email from co-author Ross Arena: “I am troubled by these accusations, as is AHA. I have included an AHA representative who will address this.” [No AHA response followed.]
A July 17 response from us noted that technically these are observations, not accusations. We “observed” that their screening policy was co-authored by the CEO of a screening company. (We offered to link them to dictionary.com to see the difference between the two words, but they declined.)
Share this:

Keas Meets Lake Wobegon: Everyone Is Above Average (in Stress)
Today we reprise the Keas Stress Survey. If laughter is the best medicine, an excellent way to reduce stress is to read this survey, using our handy guide below. Funnier still, we asked Keas all these questions below many months ago, and not only did they not answer them for us, but they didn’t even bother to correct these mistakes on their own website despite all the violations of rules of simple arithmetic. And as we have pointed out on many occasions, rules of arithmetic are strictly enforced.
![]()
You write that 41% of employees are reporting above-average stress. Shouldn’t that mean another 41% are also below average in stress? We can’t seem to find any mention of even a single employee being below average in your survey.
ANS: Refused to answer
Of those 41% reporting above average stress, you say:

So 24% of 40% of 41% are losing sleep due to work? Isn’t that 4%? So 96% of employees are not losing sleep due to work. Isn’t this a good thing?
ANS: We didn’t even bother to ask

You say 72% of women experience above-average levels of stress while only 28% of men do. Since women comprise nearly half the workforce, shouldn’t those two figures weight-average out to nearly 50% rather than 41%, assuming you sampled correctly?
ANS: Refused to answer
If indeed only 28% of men report above average levels of stress, doesn’t that imply that 72% of men aren’t unduly stressed and therefore stress reduction for men need not be a corporate priority?
ANS: Refused to answer
You say high stress “causes” many diseases, but every disease you list except depression affects more men than women. Doesn’t this claim that stress causes these diseases contradict your finding that women are three times as stressed as men?
![]()
ANS: Refused to answer
You also claim that high stress levels can also “worsen” a “myriad” of conditions? If that were indeed the case and women have three times the stress of men, how is it that women live five years longer than men?
ANS: Refused to answer

You use the words “average” and “normal” with regard to stress as synonyms, but aren’t they often antonyms? While all of us want our kids to be normal, are you aware of anyone who wants their kids to be average?
ANS: Refused to answer
Just like in Garrison Keillor’s Lake Wobegone, where all the children are above average, is the goal of your anti-stress recommendations to reach a point where everyone’s stress is below average?
ANS: Refused to answer
![]()
Should you be advising people to take Vitamin C pills when the Mayo Clinic is advising not taking them? Where is the peer-reviewed major journal evidence that Vitamin C pills reduce stress for people who, like most employed Americans, already get adequate Vitamin C?

ANS: Refused to answer
Can you point us to the objective evidence that says that unhealthy employees can be “fixed,” especially using a stress-reduction program?
ANS: Refused to answer
How much of the additional 36% that “employers at large companies” are paying for healthcare now (vs. five years ago) is due to an increase in medical events in the disease categories that you say are caused by stress? How do you reconcile that statistic with the Agency for Healthcare Research and Quality’s (AHRQ) database indicating that inpatient medical event rates in the disease categories you listed have declined over this five-year period?
ANS: Refused to answer
Likewise, how do you reconcile that 36% increase statistic with the AHRQ’s database finding only about 7% of medical spending is due to inpatient events in those categories you say are caused by stress?
ANS: Refused to answer

If companies “where health is actively promoted are three times more productive,” does that mean that a wellness program would allow pilots to fly three times faster? Could class sizes be increased from 20 to 60? Could doctors cure three times as many patients? Could police arrest three times as many criminals? Could customer service recordings could tell us our calls were three times more important to them?
Could Walmart could run its stores with a third as many employees if they were actively told to get into better shape?
ANS: Refused to answer
More importantly, wouldn’t a two-thirds reduction in staff increase stress on the remaining employees, which is exactly what you are trying to avoid?
ANS: Refused to answer
Share this:

Healthstat Wipes Out Disease
Healthstat
Short Summary of Company:
“The men and women directly involved with improving employee health are at the heart of Healthstat’s singular commitment to wellness. Healthstat’s wellness-minded practitioners establish a more personal relationship with employees, while bringing a combination of compassion and expertise to employers’ existing healthcare programs.”
Materials Being Reviewed
Case study of Mt. Vernon Mills, in which Healthstat reports more than $2000/person/year in savings through risk reduction and mitigation.
Summary of key figures and outcomes:
 Questions for Healthstat:
Questions for Healthstat:
You are claiming savings well in excess of $2000/person by Year 5, including fees. Since the average person only spends about $2000 on total hospitalizations (excluding birth events), wouldn’t this mean that you wiped out hospitalizations?
ANS: Refused to answer
The average person in an older workforce only spends about $200/year on wellness-sensitive medical events, offset by program fees and preventive expenses. How are you able to save $2000/year when there is only $200/year available to be saved from totally eliminating these events?
ANS: Refused to answer
What is your wellness-sensitive medical event rate for this population? If you don’t track it, why don’t you track it?
ANS: Refused to answer
Is it possible that since instead of comparing rates of wellness-sensitive medical events that you compared forecasted costs to actual costs, that mis-forecasting the costs is responsible for most of the improvement?
ANS: Refused to answer
You displayed the “top 20%” and “top 50%” to show their improvements. Would it be the case that had you displayed the bottom 20% and bottom 50%, their readings would have deteriorated over the period?
ANS: Refused to answer
How did you account for dropouts and non-participants, who presumably would not have shown good results and whose wellness-sensitive medical events might have increased?
ANS: Refused to answer
How can you reduce costs through wellness programs by $2000/year if cholesterol and blood pressure barely improved, even without offsetting those improvements with dropouts and non-participants?
ANS: Refused to answer
Date: June 16-21, 2014
Addendum: Email exchange
Healthstat:
Your questions do talk about wellness and savings, but do not necessarily focus on how our business model works. Therefore, they don’t make sense for us to answer them in the way they are presently written. We work with an insurance free onsite employee wellness center model that is HRA and preventative wellness driven. Our cost savings are calculated from an insurance premium cost estimate for self-insured companies, as well as preventative treatments for those potentially at risk for more costly services.
They Said What? response:
Based on your website, and also your email, you say you have a model that is “an employee wellness center” that is “preventative wellness driven” and you provide “preventative treatments for those potentially at risk.” The questions are therefore quite pertinent in regard to your business model and boil down to one: How does your “preventative wellness model” reduce wellness-sensitive/risk-sensitive medical events by $2000/person/year, when most companies only spend $200/person/year on wellness-sensitive medical events in the first place?
Share this:

HealthFitness takes credit for program savings without having a program
HealthFitness
Short Summary of Intervention:
“When you partner with HealthFitness, we work collaboratively with you to develop a strategic plan for program implementation, which includes a cultural assessment and an operational plan. You can expect results-oriented programs and services delivered through a highly personalized strategy, matched to your employees and culture.”
Materials Being Reviewed:
Success at risk reduction and translation of that risk reduction into cost savings. These excerpts are from the successful Koop Award application at http://www.thehealthproject.com/documents/2011/EastmanEval.pdf.

Summary of key figures and outcomes:
- Reduction in risk factors from 3.20 to 3.03 — net change of 0.17 — over 5 years. This success excludes dropouts.
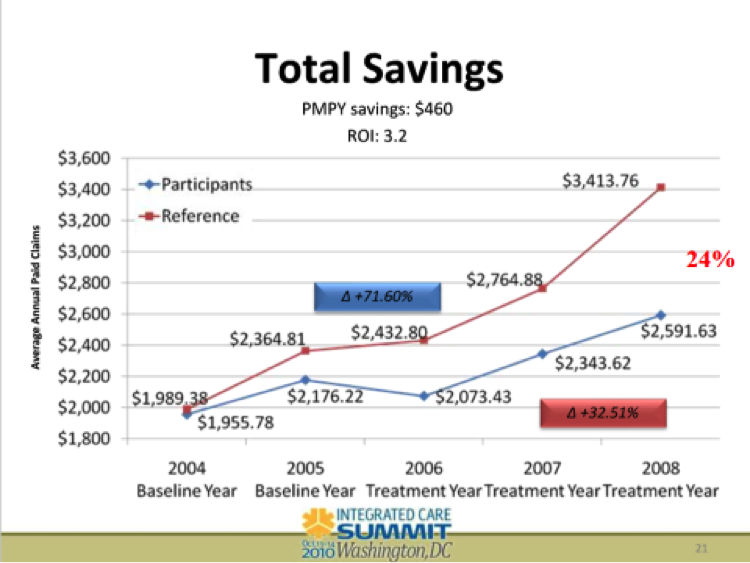
- 24% improvement in costs vs. non-participants, or $460/year at Eastman Chemical (currently up to >$500/year according to HFC website)
Questions for Health Fitness Corporation:
Since only about 20% of all inpatient events are wellness-sensitive, and you only reduced risk factors by 0.17 per person, and hospital expenses are at most 50% of total spending, how is it that you are able to reduce spending by 24%?
ANS: Refused to answer
Why did you take credit for savings in 2005, even though according to your own slide you didn’t have a program in 2005?
ANS: Refused to answer
Does starting the Y-axis at $1800 instead of $0 create the illusion of greater separation between the two cohorts?
ANS: Refused to answer
Your website says that comparing participants to non-participants “adheres to statistical rigor and current scientific standards for program evaluation” and “is recognized by the industry as the best method for measurement in a real-world corporate wellness program.” Can you explain how non-motivated non-volunteers who decline financial incentives to improve their health are comparable to motivated volunteers, especially in light of the separation between the two groups that took place just on the basis of differential mindset in 2005, before you had a program?
ANS: Refused to answer
You and your customers have won three Koop Awards in the last 4 years. Do you think also being a sponsor of the Koop Award (along with Eastman, in this case) has helped you win these awards or is this just a coincidence?

ANS: Refused to answer
Why Nobody Believes the Numbers defines the “Wishful Thinking Multiplier” as “alleged cost saviings divided by alleged risk reduction.” Your cost savings is $460 and your risk reduction in 0.17, for a Wishful Thinking Multiplier of 2700, the highest in the industry. The book calculates that a risk reduction of your magnitude (even assuming dropouts also reduced risk by the same amount) could generate roughly a $8 reduction in annual spending. To what do you attribute your ability to reduce spending by 50x what is mathematically possible?
ANS: Refused to answer
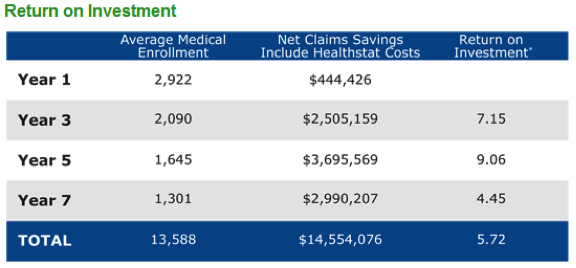
Help us with the arithmetic below, also from this Koop Award application.

How is it mathematically possible to have a higher ROI ($3.62) when also including the cost of incentives in program expense than the ROI ($3.20) excluding the cost of paying incentives to employees to participate?
ANS: Refused to answer
Update December 2014: Ron Goetzel admits HFC lied. (See #5 and #6.) The slide was “unfortunately mislabeled,” using the passive voice, as though it was an act of God (“the game was rained out” ) or else perhaps the North Koreans. The geniuses at HFC apparently didn’t notice this “unfortunate mislabeling” for 4 years, despite it’s having been pointed out to them many times before this.
Share this:

Health Fitness Corp wins a Koop award for curing non-existent cancers in Nebraska
C. Everett Koop National Health Award Committee,
Wellness Council of America and Health Fitness Corp.
Short Summary of Award:
The C. Everett Koop award committee’s mission is:
“…to seek out, evaluate, promote and distribute programs with demonstrated effectiveness in influencing personal health habits and the cost effective use of health care services. These programs have the objectives of
- Providing appropriate quality care
- Sharply reducing the alarming rate of health care inflation, by holding down unnecessary expenditures.”
Materials Being Reviewed:
The brochure in question describing the Nebraska program is downloadable from the WELCOA website.
Case Study of Award Winner for 2012: Health Fitness Corporation and Nebraska
Summary of key figures and outcomes:
Alleged cancer outcomes include the following:
Risk reduction outcomes include the following:

Questions for C. Everett Koop Award Committee:
I: Alleged Cancer Outcomes
Were you troubled by the program sponsors’ decision to waive all age-related colon cancer screening guidelines established by the government, and send out 140,000 flyers, at taxpayer expense, featuring a beautiful woman much too young to have a screening colonoscopy?
ANS: Refused to answer
How come, when the program reported that 514 of the 5000 (or fewer) people screened had colon cancer (in addition to the ones who would have been screened anyway), none of the Committee members with health informatics backgrounds from Truven Health Analytics and Mercer and Milliman (and from Wellsteps and Staywell, both of whose programs are also highlighted) were concerned that this alleged 11% colon cancer rate was at least 100 times greater than Love Canal’s?
ANS: Refused to answer
When Health Fitness Corporation admitted lying and reversed their story from making “life saving, cost-saving catches” of “early stage [colon] cancer” to revealing that those 514 people didn’t have cancer, why did the Koop Committee re-endorse what would appear to be outright data falsification, instead of rescinding the award?
ANS: Refused to answer
Even if the committee is allowing Health Fitness Corporation to keep its award and not even apologize, why does this claim of “life-saving, cost-saving catches” still appear on the WELCOA website even though the lie has been admitted?
ANS: Refused to answer
Wouldn’t the fact that the perpetrator of this acknowledged lie is also a sponsor of this Koop award that its own customers have won three times (including this incident) create the perception of a conflict of interest?

ANS: Refused to answer
Does anyone on the Committee think if Dr. Koop were still alive that he would endorse your position on data falsification of cancer victims?
ANS: Refused to answer
WELCOA’s website said it was founded by someone who appears to be the inventor of the self-serve all-you-can-eat restaurant. Despite his well-deserved reputation for integrity, did he endorse data falsification of cancer victims even after the perpetrators admitted it?

ANS: Refused to answer (but did change the spelling)
II: Risk Reduction Outcomes
How do you reconcile the claimed savings figure exceeding $4-million with your own chart above showing that only 161 active participants (3.1%) reduced a risk factor? (That chart of course doesn’t include dropouts and non-participants, whose risk factors may have increased.)
ANS: Refused to answer
Dividing the total savings by 161 yields more than $20,000/person in savings. Wouldn’t that $20,000+ for each risk factor avoided imply that all 161 would have had a heart attack even though the entire eligible population only had about 30 heart attacks the previous year, while the participating population would have had about 7?
ANS: Refused to answer
How do you reconcile your statement that 40% of the population had previously undiagnosed high blood pressure or high cholesterol with your other statement that “the total number of prescription scripts [sic] filled within the Wellness Plan reduced [sic] 3% last year,” despite your reducing or waiving the copays? Shouldn’t prescriptions have gone up, if indeed 40% more people were at risk?
ANS: Refused to answer
How can you attribute the 3% reduction in prescriptions to “improved lifestyles” with the fact that your own graph shows only 161 people improved their lifestyles enough to reduce a risk factor? What happened to the thousands who were diagnosed but were neither medicated nor improved their lifestyles?
ANS: Refused to answer
How do you reconcile that same finding – that 40% had high blood pressure or cholesterol — with that same graph, showing that almost three-quarters of the population was low-risk?
ANS: Refused to answer
How do you reconcile the brochure’s claim that the “majority of employees touted how the program has improved their lives” with the brochure’s own admission that only a minority of employees (42%) even bothered to be screened once and only 25% twice despite the four-figure financial incentive?
ANS: Refused to answer
Follow-up response
Not-for-attribution response received August 1, stating that the reason the Committee let them keep their award was not because were a sponsor but rather because they did not make the life-saving claim on their application. (They did make all the other invalid claims.) Because they didn’t make the claim on the application, they are not in violation of the Committee’s ethical standards by making it in other venues.
Our reaction:
So it is OK if a ballplayer admits using steroids as long as he didn’t happen to test positive?
Follow-Up Response
September 2014: Nebraska listed as a “best practice program” by Ron Goetzel
Our Reaction:
Doesn’t this listing contradict your initial excuse — that you forgot to ask them about whether they made up their cancer statistics during your due diligence — because now you know about that lie and all the other lies in their outcomes measurement…and yet you still call them a best-practice program?
Share this:

Better health guaranteed by CIGNA…maybe not
Cigna
Short Summary of Intervention:
Risk reduction program aimed at high- and medium- risk employees. Cigna guarantees that a significant percentage of that high- and medium-risk population will reduce risk factors over the next twelve months.
Links to Materials Being Reviewed:
This is the short version of the brochure and this is the long version. 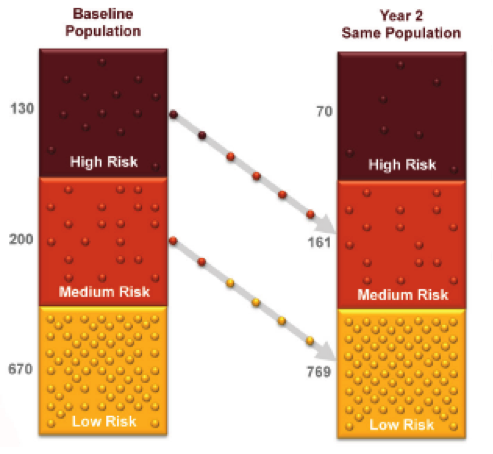
Summary of key figures and outcomes:
30% of high- and medium-risk members will reduce their risk factors in the ensuing 12 months. (Note: the actual guaranteed figures have varied in the past and may today be different from what you are reading here. However, the concept is still the same.)
Questions for Cigna:
According to noted wellness authority Dee Edington, whose slide is reproduced below, there is a natural flow of risk in a population, so that many high- and medium-risk people would reduce risk factors on their own even absent a program, while some low-risk people might increase their risk factors. How does your Better Health Guarantee adjust for that?
ANS: Refused to answer  It appears from this bar chart that low-risk people account for two-thirds of a population, and yet only one-third of the bar chart. Why did you elect not to draw these segments to scale, in keeping with the tradition of bar charts being drawn to scale?
It appears from this bar chart that low-risk people account for two-thirds of a population, and yet only one-third of the bar chart. Why did you elect not to draw these segments to scale, in keeping with the tradition of bar charts being drawn to scale?
ANS: Refused to answer
On that same chart, there is no indication that any of those two-thirds (670 out of 1000) might increase their risk factors, perhaps by regaining weight previously lost. How does your Better Health Guarantee account for the likelihood that people might regain weight or resume smoking?
ANS: Refused to answer
Speaking of which, let us assume that there is only one risk factor, smoking. Let us also assume that everyone in my organization smokes half the time, but they also quit half the time. Wouldn’t your Better Health Guarantee methodology show a 100% decline in smoking every year even if you don’t do anything and the actual rate of smoking remains the same every year?
ANS: Refused to answer
Share this:

Dr. Aetna Will See You Now
Aetna
Short Summary of Intervention:
“Aetna is launching a pilot program to test the benefits of new FDA-approved, prescription weight-loss drugs combined with lifestyle support. – See more in this news release.
- Aetna Press Release
- ”Special Communication” in JAMA Internal Medicine, published by the American Medical Association
- Aetna Presentation April 17
Summary of Aetna’s key points:
Self-insured employers can sign up for this program in which Aetna will outreach to obese employees and recommend use of the drugs Belviq and Qsymia
Questions for Aetna:
You are only offering this program to self-insured employers. If this is, as your title says: a “strategy to improve health status and reduce costs,” why are you denying this program to your own fully insured members, where the cost savings would accrue directly to your own shareholders while the health status improvements would benefit your own members?
ANS: Refused to answer
Does it concern you that neither drug in your pilot is approved in Europe and that JAMA Internal Medicine says the drugs have been associated with serious harms and that these well-respected JAMA physician editorialists state that these drugs should not have been approved for use in the United States?
ANS: Refused to answer
How does your description of these drugs on your sales slide as “safe and effective” square with the question above?
ANS: Refused to answer
Why, over the course of the 70-minute webinar (for which attendees were charged $300), didn’t you mention the JAMA essay or any other safety concerns?
ANS: Refused to answer
In addition to omitting mention of the potential harms in the JAMA article, none of your materials mention that the (many) known side effects include impacts on memory, attention and language. Wouldn’t those side effects be of concern to an employer who is interested in, as your materials say, increasing the productivity of the employees taking the drugs?
ANS: Refused to answer
Does it concern you that these drugs have been by and large rejected by patients and physicians, with sales for Belviq “well below even reduced Wall Street expectations” while Qsymia has been described as ”flailing” ?
ANS: Refused to answer
Does it concern you that, of any drug on the market, Belviq has the highest ratio of payments to doctors to overall sales?
ANS: Refused to answer
Suppose an employee’s doctor won’t prescribe these drugs. Many doctors refuse to prescribe these drugs because of the side effect profiles (hence the very low sales figures). In that case, will you pressure the doctor to prescribe the drugs, get a list from the manufacturers of doctors in the area willing to prescribe the drugs and encourage the employee to switch doctors, or pressure the employer to tell the employee to drop out of this program they were just recruited into at your request? In other words, if the doctor doesn’t comply, will Aetna play doctor?
ANS: Refused to answer
Are you aware of any other health plans that will recommend name-brand drugs to members who call and say that they have obesity or any other disease?
ANS: Refused to answer
Are you aware of any other health plans that, rather than wait for members to ask for drug recommendations, outreach to members who have a disease in order to recommend proprietary name-brand drugs?
ANS: Refused to answer
Are you aware of any other health plans that outreach to members who do not have a disease, but only a high BMI, to recommend proprietary prescription drugs, especially prescription drugs that “have been associated with serious harms”?
ANS: Refused to answer
You said on your webinar that people who go off these drugs will “gradually regain weight.” In that sense, other than the $2400/year cost and “potential for serious harm,” how would this result different from any other diet, in that people who stop adhering carefully will gradually regain their weight?
ANS: Refused to answer
Any responses, apologies, retractions, changes etc. by the vendor are listed here:
June 23, 2014: Note from Ed Pezalla at Aetna, Vice President for Pharmacy Policy and Strategy: “Thank you for reaching out and inviting additional dialogue. We have a new article about the program that addresses many of your questions. We expect to publish the article in the next week or so in Aetna’s Health Section. I can send you a link once it is posted.”
August 11, 2014: Ed Pezella sent an article that would “answer some of the questions“. I am having trouble locating the answers in that article but perhaps that’s because I can’t find my reading glasses.
October 2015: Qsymia sales still “flailing.” May be off the market by 2017. Belviq struggling as well. Aetna could have avoided this entire embarrassment in the first place if they had simply asked us if pitching obesity drugs to its customers was a good idea. Come to think of it, they didn’t have to ask us. They could have asked anyone with an IQ over 80.
May 2016: STATNews finds that obesity drugs — specifically these two — have been abject failures in the marketplace.
