
Home » 2019
Yearly Archives: 2019

Was Livongo’s “peer-reviewed journal article” really just an ad?
Here’s how an ad gets published. It’s a two-step process. I will lay it out so that even the dumbest member of the media who somehow missed this the first time when they swooned over Livongo’s outcomes can understand it now:
- Your employees and their colleagues write it.
- You pay to have it published.
Now, let’s look at what Livongo just published, touting their own outcomes, to see how, if at all, it differs from an ad.
- Their employees and colleagues wrote it.
- We covered this last time we wrote about Livongo. The article was written by Livongo employees, assisted by Eli Lilly employees. (Eli Lilly funded the study.)
- They paid to have it published.
- We missed this the first time around. Our excuse is, so did quite literally everyone else who covered the story. And “covering stories” isn’t our Day Job. We aren’t journalists. We don’t even play them on TV. We’ve never even watched journalist shows on TV, unless you include Superman reruns. Livongo seems to have a lot in common with that show, transparency being their kryptonite.
The journal is called the Journal of Medical Economics. Sounds really prestigious, so points for that. Yet virtually no other journal article cites articles in this journal, giving it an Impact Factor south of 2. (New England Journal of Medicine gets a 70.) Turns out there’s a reason no one cites it. Here’s how you get published in it. You pay them money.

They would say, yes, but we got it peer-reviewed. To which I say, apparently you didn’t in any meaningful sense. A real peer reviewer would have found and questioned all the fallacies in their article, rather than rubber-stamp some very sketchy “findings,” which for convenience’ sake are all catalogued in one place.
There is nothing wrong with advertising your outcomes, as long as your ad is labeled as an ad. You often see airline magazines with entire sections advertising various cities, using articles and pictures. But they are always labeled as ads. If you don’t do this, there is always the slight possibility, however remote, that someone doesn’t do the research to figure out that in fact this publication was pay-to-play. If that were to happen, you might see a headline like this:

Whereas a more accurate headline might read: “Livongo Pays for an Article to Claim Its Product Works.”
Update January 3: Someone contacted me to say that the correct term for paid highly information advertising is “Sponsored content.” This term would apply perfectly to Livongo’s self-generated, self-published study. They should relabel it as such.
Share this:

Surprise billing legislation blew up yesterday!
Surprise billing legislation blew up yesterday.
This means as we enter the 2 weeks with the most emergencies this side of July 4, you are at risk of being snookered in an emergency admit or visit or delivery. However, you can now download this consent language and instructions on use right into your Apple Wallet (sorry, Android users — not your day in the sun yet)
The same link has our paper version, with 8 wallet-sized cards. Print the page and slice it into 8 cards. (The good news is that since the ER can’t overcharge you if you carry these cards, you don’t even have to be careful with the scissors.)
Share this:


Announcing the 2019 Not The Deplorables Awards
This year we are not naming winners of the Deplorables Award, lovingly bestowed in the past on vendors best exemplifying the wellness industry’s commitment to cluelessness. This is largely because wellness vendors have finally learned to operate in the shadows. Of course, the usual suspects — previous, multiple Deplorables Award-winners like Interactive Health and Wellsteps — are still fabricating outcomes and harming employees. The difference this year is that they have finally learned that snookering employers works best if they don’t actually announce that they are snookering employers.

They have enough sense not to engage, so as not to create a news cycle…which they will invariably lose. For example, watch how Ron Goetzel won’t respond to this:
“Ronald, I’ve documented 14 statements you made in one 45-minute period that look an awful lot like lies. Care to clarify or dispute any of them? If not, we’ll assume they are lies.”
And if you look in the comments below, or on linkedin, you’ll see…nothing.
One might wonder why this simple lesson has taken these people so long to learn, but in their defense it could be noted that many politicians have yet to learn it at all.
Diabetes vendors, Livongo in particular, have proven to be faster learners. They figured out that if data goes in the wrong direction, you simply don’t report it. No one other than yours truly here will notice, and I can’t highlight their failures if they don’t blab them. Specifically, the two most important outcomes metrics in diabetes management are insulin use and primary-coded diabeties admissions. While they reported some rather contradictory and squirrelly “results” for other things, somehow they “forgot” to report on those two variables.
As a result, all the media attention directed at them has been of the reprint-the-press-release variety rather than the Woodward-and-Bernstein approach. I tried to add my two cents but didn’t get sufficient attention because Livongo was wise enough not to voluntarily disclose the self-incriminating data.
Now for the good news: many organizations and individuals have distinguished themselves this year by actually adding value — basically doing the opposite of what Deplorables Awards winners do. It’s been so long since I’ve reported good news in this column that I’m not sure what the opposite of “Deplorables Awards” is? The opposite of Deplorables might be “Human Scum,” but upon careful consideration, deliberation, and focus-grouping, I’ve decided that might not be an appropriate name for an award.

So I have no idea what to name these awards collectively, other than Not The Deplorables Awards. (And a few awards below have their own monikers as well.)
Note that it isn’t enough to be on the right side to earn this accolade — you have be high-visibility too, and willing to take public stands that might get some people annoyed with you.
And the envelopes, please
First, the Validation Institute. “Are you validated by the Validation Institute?” is becoming a common phrase. (It helps that their most recent webinar attracted 1300 registrants.) Some organizations, like Comcast, won’t even consider a non-validated vendor that can’t explain why validation doesn’t apply to them.
Some vendors will respond: “We don’t need to be validated because we hired an actuary to validate our outcomes.”
Here is a newsflash: The sentence: “My client saved no money at all” has been announced by no actuary ever. You pay an actuary to claim savings, not to measure them. This is true matter how obviously they are fabricated.
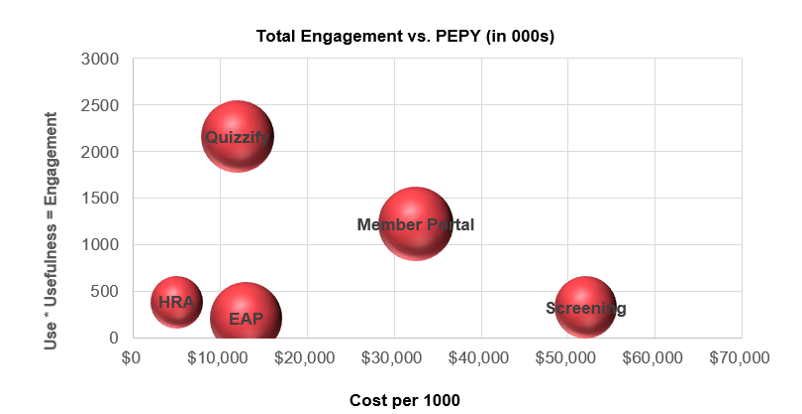
The VI has also created the single most elegant, easily implemented, and valid tool to measure the cost-effectiveness of various benefits. No tool has ever done that at all, let alone freely and easily. You simply ask employees “How many times if at all did you use this benefit?” and “Was it useful?” Multiply those two scores together to get an engagement index and graph that against the cost of the benefit. The most cost-effective benefits will demonstrate high engagement at low cost, in the upper left. (The size of the bubble scores an optional third question: “Does offering this benefit enhance corporate culture?”)
Second, the companies that have achieved validation. While many companies have now reached this milestone, these awards would specifically go to Virta and IMHealth in diabetes and US Preventive Medicine in wellness. The reason is that they have achieved legitimate outcomes in industry segments in which most of their competitors have not.
Third, Quantum Health would get the Cal Ripken award, for six consecutive years of winning validation at the highest level, which is actual savings achieved.
Fourth, the authors, of which there were no shortage this year:
- The John Dean award goes to Professors Zirui Song and Katherine Baicker, who did exactly what scientists are supposed to do, which is design, conduct and report legitimate experiments instead of fudging the data to show that their initial conclusion — in their case, certainly the most consequential initial conclusion ever — was right. By proving that “pry, poke and prod” is an epic fail (at least for the first year, and it’s hard to imagine a dramatic turnaround in subsequent years), they did the honorable thing, even though it meant invalidating their own previous work.
- The Hire-a-Food-Tester award goes to Marty Makary, whose blockbuster The Price We Pay exposed some mind-bogglingly scandalous behavior by providers harming employees with surprise medical bills and lawsuits. Runner-ups in the authors-of-actual-books department (only because Marty’s is tough to beat) include Jeanne Moore and Zeev Neuwirth.
- Marilyn Bartlett wins the Miss Noncongeniality Award for forcing most of the hospitals in Montana to accept reasonable fees benchmarked to Medicare, saving the state tens of millions. Were she to help other states achieve the same outcomes, the complexion of the entire provider industry would change. Large private-sector employers, and carriers, would start demanding the same rates.
- Joe Andelin, who has published several analyses blowing up conventional wisdom about savings from wellness.
- Lisa Woods, Jonathan Slotkin, Ruth Coleman for documenting mind-blowing rates of inappropriate spinal fusions
- Medencentive, whose published analysis combined both validity and savings, which (aside from Quantum Health) has never happened in employee health services
Fifth, the Joe Hill award to AARP, for representing low-paid hourly workers being abused by Yale University’s wellness program. “Abused” may seem like a strong word, but forcing an employee who has had a double mastectomy to choose between getting a mammogram or being fined up to $1300 might qualify as such.
Sixth, the Tesla 0-to-60 Award goes to Tom Scott, who, from a standing start at the 2018 World Health Care Congress, created the first and most popular full-credit, full-semester course on next-generation health benefit design and administration.
Seventh, the Jacob Riis Award goes to Jon Robison, who never misses an opportunity to point out the fallacies in wellness vendor claims. Those pile up so fast it’s amazing he has time for his Day Job.
Eighth, the Edward R. Murrow award to the podcasters. Podcasts are the new way of reaching people, and exposing “pry, poke and prod” programs seems to be a popular topic. In no particular order, they are Reconstructing Healthcare, Workplace Injury Prevention, Stacy Richter, Josh Luke, Jen Arnold, Zeev Neuwirth, Jeff Bernhard, Michael Andrade, Matt Jeffs.
Then, in the not-really-a-podcast category, hosts who get the message across in 3 minutes or less include Fred Goldstein and Wellable’s NIck Patel.
NInth, the First Amendment Award goes to Brian Klepper. Brian has compiled a listserve of almost 1000 disruptors where folks like me learn we are not alone in the universe. To join the listserve, you can reach Brian at brian.klepper@validationinstitute.com.
Tenth, the Grownups in the Room. These are people who, despite running high-visibility organizations that are susceptible to criticism, are completely willing to take unpopular stands when the facts merit it, and have clearly moved the needle.. Leah Binder, Chris Slezak, Jessica Brooks, Neil Goldfarb, Christie Travis, Lisa Morgan, Larry Boress, Bob Smith, Lisa Slavinski, Tina Bowling, Jeff Hogan.
Eleventh, the Nero Award goes to…me. Not for the things I generally excel at, like measuring wellness outcomes, writing heathcare trivia questions, or being tall. Rather, specifically for combining the insights of the aforementioned Marilyn Bartlett and Marty Makary into the first-ever on-the-spot solution for avoiding surprise medical bills for emergency care. The good news is that, following our heavily subscribed webinar (viewable here) on this topic, several hundred people have downloaded this solution. The bad news is, that means several hundred million people haven’t.
And, finally, what would a list of Not the Deplorables Awards be without: The Daves? Dave Chase and David Contorno have used their bully pulpits to influence large numbers of brokers to negotiate better deals on behalf of their customers that also dramatically reduce deductibles and copays. Mr. Contorno’s latest linkedin post got more than 200 “likes,” which implies about 50,000 views. Remind me never to get on his bad side.
By contrast, I am thrilled to be on Ron Goetzel’s bad side. And in all fairness, he has responded to the 14 apparent lies. Not by disputing them (which is what I am offering the chance to do now) but by acknowledging them. The only point he disputed, in the comments, was a true statement. He said on tape he found Quizzify to be “a lot of fun, very clever.” But now he claims that when he said that, he didn’t mean it.
Make that 15.
PS I think you can order both t-shirts from the same company. Is this a great country or what?
Share this:


Life imitates The Price We Pay
If there’s one thing you learn from Marty Makary’s blockbuster expose The Price We Pay (other than Quizzify being a great vendor, on page 226), it’s not to get a peripheral vascular screen at a community center.
Here are his exact words from his trip to a community center hosting a screening session for peripheral vascular disease:
The person from the cardiology group was conducting a test that measures how the blood flow in the legs compares to the blood flow in the arms. The rationale: Something might be wrong if the blood pressure is lower in the legs. It could be caused by a narrowing of the arteries, a plaque that slows blood flow. It might warrant further investigation.
There’s just one problem with that notion: This test should not be performed unless a patient has serious symptoms, like crippling leg pain. For anyone else, it’s likely to lead to medical care they don’t need, which can be expensive and dangerous. That’s exactly why independent medical experts do not recommend the type of peripheral vascular screening I witnessed that day.
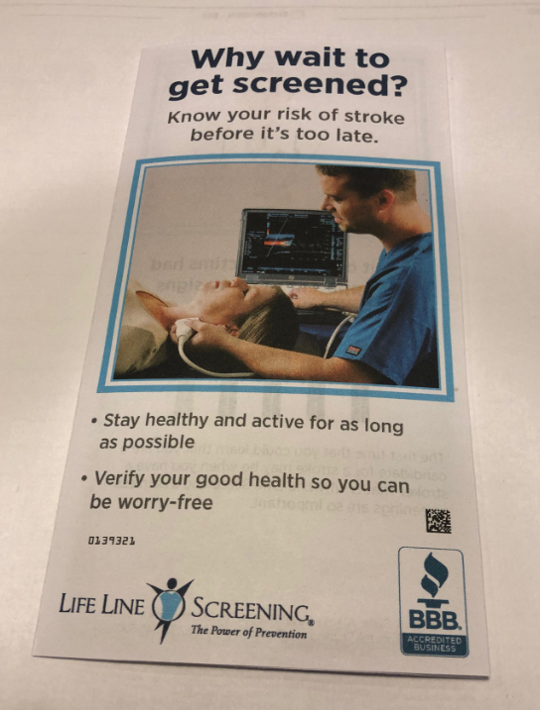
So, thanks to the chronic shortage of other subject matter for these periodic blogs now that wellness vendors have finally learned not to brag publicly about their stupidity, imagine my glee when a brochure from Life Line Screening arrived in the mail last week urging me to: get peripheral vascular screening at a community center.
Not only that, but my special “priority code” meant I “qualified” for a large, exclusive, discount (“Only $149”). I was very pleased to hear that — just like achieving Mosaic on JetBlue, Titanium Ambassador in Marriott, and something like Executive Platinum Emerald Diamond Palladium Plutonium Selenium Sodium Fluoride on American — I had also achieved “Status” with Life Line.
Needless to say I wanted to brag about this achievement to all my friends-and-relations who also got this mailing. But my ego took a hit when I learned that apparently they too received high-priority codes and qualified for this exact same exclusive discount. Trying to figure out what we all had in common to earn this special treatment, we concluded that this it was being offered — exclusively — to people who are comprised of protoplasm.
In addition to the peripheral vascular disease screening, rated “D” by the US Preventive Services Task Force in my 40-64-year-old group, they are offering the following additional “vital screenings,” with the USPSTF rating in parentheses:
- Abdominal aortic aneurysm screening (D for nonsmokers under 65)
- Heart rhythm screening (I rating)
- Osteoporosis (I rating)
- Carotid artery screening (D rating)

For those uninitiated in USPSTF screening ratings, “D” means “don’t screen for this,” because of the overwhelming likelihood that positives will be false.
How overwhelming is this likelihood? Let’s take an example. Suppose you perform a test that’s 90% accurate to hunt for a previously undetected, symptomless, disease in 1000 people. Suppose further that about 1 in 1000 adults 40 to 64 has this undetected disease. A 90% accurate test is also 10% inaccurate. So, including the one person who actually has the disease, about 100 of the other 999 will test positive — despite being disease-free.
Those 100 are going to be totally stressed out for no reason, probably follow up with more tests, and possibly even get surgery. Here is the math:
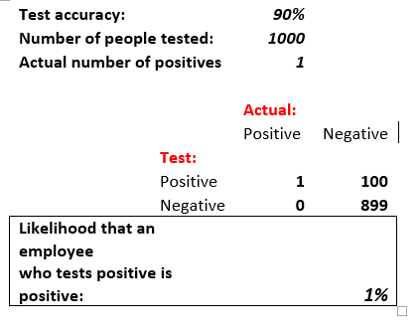
Continuing with my USPSTF grading lesson for Life Line, “I” means “Incomplete,” not enough data for a recommendation. I don’t have to tell you what “A” and “B” mean because those ratings don’t apply to any of Life Line’s screens. That’s right. None of Life Line’s tests are recommended by the specific entity charged with recommending tests.
Needless to say, I couldn’t pass up the opportunity to call these Very Stable Geniuses. My call was answered by a Life Line employee who announced: “My name is XXXX. I’m going to be your Preventative Healthcare Advisor.” When I asked if these tests had an A Rating from from the US Preventive Services Task Force, she replied: “Very very very true. Also an A-Plus rating from the Better Business Bureau.”
She also assured me I could keep my clothes on, which I know the staff and guests of the Wellesley Community Center will appreciate.
The benefits of screening

Hmmm. Let’s look at each of these five claims in turn.
- “Early detection.” Check. Detection of more false positives than every wellness vendor except possibly Interactive Health, which specializes in them. (See “Interactive Health gives clueless wellness vendors a bad name.“)
- “Prevention of disease progression.” Screening might possibly detect something but it doesn’t prevent anything. Here’s what might prevent something: spending that $149 on a new pair of sneakers and running in the opposite direction of the Wellesley Community Center.
- “Peace of mind.” Try telling that to all the people who are getting false positives.
- “Savings with more affordable screenings.” I called my Preventative Healthcare Advisor to ask about that one. Turns out, as noted below, I can practically retire off these savings.
- “Control, no insurance required” ? “Required” is synonymous with “coverage” in this case. Just like “true” was synonymous with “false” about the USPSTF A ratings.
So…doctors don’t do these screens, insurance doesn’t cover them, and yet somehow, somehow, these screens are… “vital“? Time for another call to my preventative healthcare adviser to find out why, if these tests are so vital, doctors don’t do them. She explained that:
- Doctors will only do these tests for: “a reason” (shame on doctors!)
- But by then it might be “too late.”
- Doctors don’t do these tests routinely because they cost “$5000 to $8000,” instead of $149. That’s why the brochure lists “savings” as a benefit. You could save thousands right now by doing these screenings! Likewise, think of all the money you’re saving this month alone by not living in a $5000/month apartment.
- “Insurance companies are all about the money. They try to control our lives. That’s why they won’t pay for these tests.” (There is actually an element of truth to this one. Insurance companies are all about the money. Not unlike Life Line, which is clearly in business for their health, since they aren’t in it for ours.)
Postscript: I did check in with a primary care physician, who observed that she’s heard of doctors doing tests without “a reason.” But advertising that they do tests for no reason? That was news to her. She said they could lose their license. I pointed out that wellness vendors don’t need licenses, or for that matter even GEDs. Just the willingness to check their ethics at the door of the Wellesley Community Center. Plus a soupcon of protoplasm.
Share this:


Last call for Thursday’s “The cure for surprise billing” webinar
Dear They Said What Nation,
Besides the minor points that your employees’ or dependents’ odds of getting one of these surprise bills are 10 times the odds of having a heart attack or diabetes hospitalization* and that unlike the latter, these bills are utterly avoidable, here are three major reasons to sign up for this webinar:
- The 1500th registrant receives a $100 Amazon gift card from the Validation Institute, assuming they attend.
- You do NOT have to “attend” the webinar to experience it. Registrants will be given the recording. But you do have to register here.
- The way to be certain this is a valuable webinar that will result in easy, major, immediate, behavior change for any employer that implements our elegant solution is that no Koop Award-winning wellness vendor has registered for it — despite the fact that Whole Foods would redeem the gift card for almost all the broccoli you can eat.
A handful of other wellness vendors have signed up. We salute them.

- Aduro
- Health Advocate
- It Starts with Me
- Maestro Health
- US Preventive Medicine
And a special Honorable Mention to Wellable for posting the Reader’s Digest version of the webinar right here.
PS If you are a wellness vendor specifically, and I missed you while scanning the ridiculously long list of attendees, ping me and I’ll add you. Or sign up now and I’ll add you.
*OK, here is the calculation. The lower bound of these odds on any ER visit or admission is about 1-in-5 for any in-network facility according to the Kaiser Family Foundation. Others pace the odds at twice that, but we’ll go with the more conservative estimate. Your covered population incurs about 240 ER visits and admissions in total. 20% of 240 is: 48 per 1000. Whereas the number of covered people who will get a heart attack or have a diabetes event is 2 per 1000.
Oh, did I say surprise bills were ten times as likely? That would make them 24 times as likely.
And yet, unlike heart attacks and diabetes, totally avoidable…
Share this:


Care to guess the odds of a surprise medical bill for an ER visit?
According to a study published in JAMA Internal Medicine, an employee’s odds of getting a surprise medical bill for an ER visit or a hospital stay exceed 40%!
Well, you might say, serves ’em right for not staying in-network.
Wrong. This study looked only at in-network visits and admissions. Thing is, in-network facilities are often staffed with out-of-network providers. I know this firsthand — I’m in a private equity fund that’s making a killing by rolling up provider practices in local markets and keeping them out of network. It’s illegal for provider practices to collude to stay out of network, but it is perfectly legal for them to merge and make a practice-wide decision to stay out of network.
So, wellness vendors and consultants, here are two opportunities you can’t refuse, that are both central to your business strategy:
- Actually do something useful for employees, as opposed to your usual scripted diatribes. Newsflash: employees already know they need to quit smoking and eat broccoli. But they don’t know how to avoid these bills.
- Prevent me from making money.
Also, this is the one thing that could bankrupt them that is totally avoidable. And yet your financial wellness program doesn’t cover it.
Fortunately, if you can spare one short hour on October 31 (which you will get back 38 hours later, when the time changes), you can learn how your employees can avoid these bills. All it takes is a little sticker to put on an insurance card and teaching employees to use their card, rather than sign whatever is put in front of them and/or say: “Same as last year” when they ask you if your insurance information has changed.
The all-star cast of this webinar includes David Contorno, Brian Klepper, Marty Makary, and Marilyn Bartlett. You can register here.
PS If you can’t make the time because of open enrollment, you’ll have access to the recording.
Share this:


WTF! Introducing the wellness industry’s Wishful Thinking Factor

Finally! A valid way to measure wellness outcomes that requires only a calculator, a triple-digit IQ, and complete suspension of disbelief! Introducing the Wishful Thinking Factor, or WTF. Those of you accustomed to reviewing wellness vendor outcomes may think those initials stand for something else…and we will indeed use those initials in their more common context at the end of this posting.
By contrast, this WTF is defined as:
Dollars claimed as savings/percent improvement in risk factors.
The elegance of the WTF is exceeded only by its widespread acceptance. WTF is already the wellness industry’s preferred analysis, so I am merely confirming that we agree. The only difference between my WTF calculation and theirs is they don’t actually put the numerator and denominator on the same page.
Meaning, they don’t actually announce: “Here’s our huge savings generated by our trivial risk reduction…wait…this is impossible…WTF???”
That’s because then it would be perfectly obvious that they are fabricating the savings. Instead they put “dollars saved” on one page and the improvement in risk factors on another page, way far away — and hope nobody compares them. (Interactive Health is the most stable genius example of that, as we’ll see below.)
What is the real causal relationship between risk reduction and savings?
A distressingly relevant joke circulated among us rip-roaringly hilarious faculty back when I taught in the Harvard economics department. A chemist, physicist and economist are stranded on a desert island with only a can of beans. To open it, the physicist suggests dropping it off a cliff, so that it will open upon impact. The chemist points out that would splatter the contents, and suggests instead that they put the can in a fire, and once the can gets hot enough, it will melt. The physicist points out that the beans would all burn up in the fire. At an impasse, they turn to the economist and ask what he would do.
The economist replies: “Assume a can opener.”
In keeping with that spirit, we will make six (count ’em, 6) equally generous assumptions for determining the true WTF:
- Every wellness-sensitive medical admission or ER visit is a direct function of the risk that the wellness vendor measures in a population. In other words, social determinants of health and genetics have nothing to do with the likelihood of a heart attack or diabetes event
- Even the dumbest wellness vendors know how to measure risk (following their five days of training in medicine)
- Employees never cheat to improve their biometric scores and never lie on their risk assessments
- Dropouts and non-participants would improve in risk at the same rate as participants do, so the fact that they don’t participate doesn’t change the overall risk reduction in the population
- No lag time between risk reduction and event avoidance
- No false positives, no added lab tests, drugs, doctor visits or anything else that might possibly increase utilization and cost of outpatient care in order to reduce inpatient utilization — which of course is the opposite of what the wellness trade association readily admits to:

Using those generous assumptions, measured wellness-sensitive medical admissions (WMSAs), and the total cost of those events, would decline at the same rate as measured risk declines. According to the Health Enhancement Research Organization, WSMAs comprise no more than $100 PEPY in a commercially insured population. So every 1% decline in risk yields a spending decline of $1.
Relaxing the assumptions above would likely reveal that this WTF is also overstated, but it has the advantage of consensus among the 60+ experts who contributed to the HERO outcomes guidelines measurement tool, so we’ll call this the Gold Standard, to which other WTFs are compared.
Now let’s make a little list of the WTFs compiled by the industry’s very stable geniuses, in their great and unmatched wisdom. Naturally, in that category, the first to come to mind are Interactive Health and Ron Goetzel.
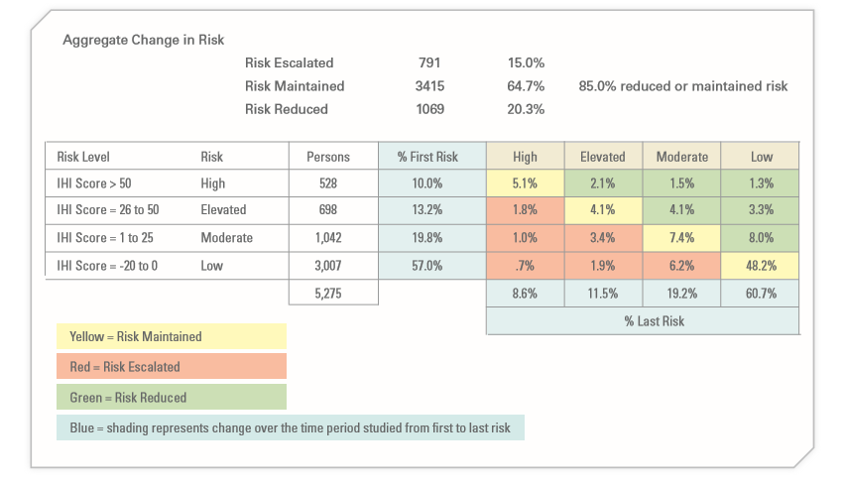
Let’s start with Interactive Health. Excluding dropouts and non-participants, they claimed a 5.3% risk reduction (20.3% reduced risk while 15% increased them). So they saved a maximum, assuming the six assumptions above, $5.30 PEPY:
The claimed savings was:

Averaging those claims yields $804, for a WTF of 151.
As a side note, allocating that $804 in savings across the 5.3% who actually did see a decline in risk factors yields over $15,000 per risk factor reduced. No mean feat when you figure that the average person only incurs about $6000 in employer spending. That was enough to get them in the Wall Street Journal
A second example (and there are many more) is the Koop Award given to Health Fitness Corporation for lying about saving the lives of cancer victims who never had cancer. The coverup of that fabrication was the lead story about Nebraska, along with whether Ron Goetzel had committed an actual crime, as opposed to simply snookering the rather gullible state, whose reaction when they found out is best described as Human Resources-meets-Stockholm Syndrome.
Mr. Goetzel defended his actions by saying that lying about saving the lives of cancer victims was overlooked by the awards committee, and what really earned Nebraska the award was saving $4.2 million by reducing 186 risk factors. Let’s calculate the WTF from that.

the absolute reduction in risk was 0.17 (1.72 to 1.55) on a scale of 7, or roughly 2.4%. That represents about 180 people out of 5199 reducing a risk factor. (Of course, the remaining 15,000 of the 20,000+ state employees dropped out and/or wanted nothing to do with this program, but that’s a different story. So much winning!)
And yet somehow, despite only 180 people claiming to reduce a risk factor, the program saved $4.2-million, or $807 apiece for the total 5199 people. That yields a WTF of 336.
Speaking of Koop Awards, The Koop Award Committee is known for its embrace of WTF arithmetic, and it’s that time of year again during which they put their very good brains on full display. For instance, they once gave an award to Pfizer for saving $9 million, or roughly $300 per employee. How did Pfizer do that? With a 2% risk factor decline. Pfizer’s WTF worked out to about 150.
As a sidebar, Pfizer’s award application includes our all-time favorite displays:
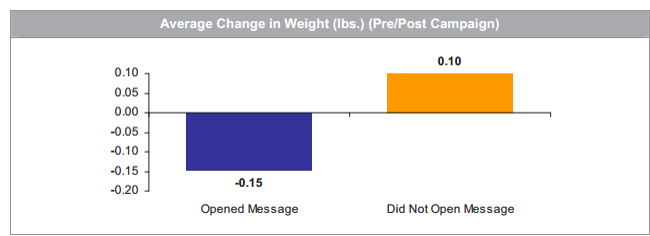
Pfizer’s wellness team sent employees emails on weight control tips. Those who opened the messages lost about 3 ounces while those who did not open the messages gained 2 ounces. That could easily be accounted for by the number of calories required to open the emails.
The 2019 Koop Award
Most recently, the very stable geniuses just gave an award to Baylor Medical School, where, in keeping with tradition, risk factors declined by a whopping 1% — at least among the 25% of the workforce willing to be screened twice (!!!) a year to earn a 20% premium reduction. Let’s take a looksee at the biometric screening results:

On average, these five categories improved 1.04%, to be exact. This is actually quite an accomplishment for the vendor, Vitality, which typically gets no improvement or a deterioration.
The claimed savings — in keeping with Koop Award tradition, buried deep on another page — were $333/year, yielding a WTF of 320.
For any readers out there with the IQs of a Koop Award Committee member, let me spell out the pattern you’re seeing: the wellness industry’s own data yields WTFs 150 to 336 times greater than the wellness industry’s own guidebook estimates.
If anyone would like to reach me to review this arithmetic, or report their own vendor’s results, contact me directly. Schedule-wise, I’m not available today (Monday) or Tuesday. However I am available later this week, specifically WTF.
Share this:


A “cure” for surprise medical billing? Webinar featuring Dr. Marty Makary
Attention, employers with wellness programs: this is bigger than broccoli.

No employee bankruptcy has ever been attributed to a broccoli deficiency. By contrast, surprise medical bills like this one are the #1 source of bankruptcies, wage garnishments and lawsuits against employees. You may have a stress management vendor and a financial wellness vendor, But their programs don’t cover the #1 source of avoidable stress related to financial wellness, for the simple reason that they don’t know how.
The Validation Institute to the rescue.
The Validation Institute is doing a webinar describing an actual cure for employee surprise medical bills for emergency visits and admits. it features the leading experts in pricing and surprise billing, including the bestselling author of The Price We Pay, Dr. Marty Makary. Here is the invitation.

October 31st webinar featuring bestselling author Dr. Marty Makary: A “cure” for employees’ surprise medical bills
You think Halloween is scary? Try surprise medical bills. That’s the subject of this groundbreaking October 31st webinar (register here).
Surprise bills may or may not be the #1 source of workplace stress – but they are certainly the #1 avoidable source of workplace stress. 57% of Americans report receiving one on the last five years. If you have not received complaints from employees about them, or noticed wages being garnished by providers, that’s probably because your health benefit is so generous that you are paying these bills without realizing it…inflating your own costs unnecessarily.
And yet there is a “cure,” at least for surprise bills related to emergency visits and admissions. The Validation Institute and Health Rosetta have assembled what they call the “dream team” of experts in pricing and consent-to-treatment to show you – in a mere hour – how to put the kibosh on this scourge. Presenters include:
- New York Times-bestselling author Dr. Marty Makary, whose blockbuster healthcare exposé, The Price We Pay, has already changed some outrageous hospital billing practices, will describe what consent-to-treatment entails, and why your employees should never just sign the forms thrust in front of them
- Industry pricing gurus Marilyn Bartlett (who saved Montana tens of millions through payment reform) and Health Rosetta-accredited broker-of-the-year Dave Contorno will provide a quick lesson in how to avoid paying inflated charges generally
- Quizzify CEO and trade-bestselling author Al Lewis will then combine these experts’ insights into an elegant one-sentence sticker to add to an insurance card that caps charges and avoids overtreatment…while ensuring employees get the care they need.
Attendees will be able to begin solving the surprise medical bills problem within weeks or even days. If you combine Quizzify’s quizzes with the solution as described in the webinar, it will do to surprise medical bills for emergency care what garlic does to vampires.
Here’s the link to the October 31 webinar registration.
Share this:

“Arithmetically impossible”: Al Lewis talks wellness outcomes with Stacey Richter
The. Numbers. Don’t. Add. Up.
Listen to the Podcast with healthcare guru Stacy Richter to find out why. Here’s what she has to say;
Employers are getting wise to a lot of things right now. I’d suggest a fast follow-on is going to be their view of these wellness programs. It will be interesting to see if current vendors are able to compete with the newer solutions that actually work and which employees actually appreciate. It will also be interesting to see if there’s any backlash against the supply chain that continues to offer up these solutions, especially given some of the lawsuits that are currently under way and all the research which is eminently available.
After about ten people wrote in looking to hear an interview with him, in this health care podcast I’m honored and pleased to speak with the one and only Al Lewis. Al is basically synonymous with wellness programs’ analysis and evaluation. One of my favorite things about Al is that he is as controversial as he is respected. He’s been called both “the founding father” of disease management, and he’s also been called the “troublemaker-in-chief” of the wellness industry. Regardless of your opinion of Al’s views, his integrity and commitment and rigorous analytical approach is open and shut. Al is the author of two books, which you can find in the show notes. He’s also the CEO of Quizzify. Quizzify is a company and an approach that teaches employees how to get the care they need while avoiding the “care” they don’t. Quizzify’s claims have been validated, by the way, by the Validation Institute.
Here’s the link. Happy listening (unless you’re an outcomes-based wellness vendor).
Share this:
Surprise medical bill of the week: $650,000 for a $7000 operation
It’s not about the broccoli, folks.
The major hazard facing employees today is not a broccoli deficiency, but rather: surprise medical bills. And here is one that boggles the mind: $650,000 for a $7000 surgery. Even when these emergencies are “covered” (meaning you pay their bill, except for the four-figure co-insurance), these bills create stress, both emotional and financial, far in excess of stress created by any problem that can be solved by eating more fruits and vegetables. The rate of these bills is also about 100 times the rate of diabetes admissions and heart attacks combined: more than half of Americans report receiving one in the last five years.
Further, people — even people who eat plenty of fruits and vegetables — live in fear of receiving one. Often one such bill can force a family into bankruptcy.
So perhaps it’s time to rejigger your wellness priorities in favor of this most pressing problem? And the other thing is, unlike risk factors (which rarely decline in a population by more than 1-2%, excluding dropouts anyway, according to the Health Enhancement Research Organization), this problem is solvable. Naturally, your wellness vendor has no clue how to solve it, so pay close attention to the following paragraph.
The “long version” of the solution can be found here, But if you don’t feel like clicking through to it, here is the short version: give your employees a sticker to put on their insurance card that says:
“I consent to appropriate treatment and to be responsible for reasonable charges not covered by insurance, up to 2 times the Medicare rate.”
Then you need to educate your employees — using Quizzify or an endless stream of memos, as you prefer — to do two things:
- Carry the insurance card and show the insurance card. It’s not enough to say: “Oh, yeah, I’m covered by so-and-so,” and have the intake person verify eligibility.”
- Do not sign the “terms and conditions” they thrust at you. That boldfaced sentence above contains the consent language needed. They have to treat you, based on that consent.
Unlike attempting to create a more broccoli-centric workplace, this is exactly the type of behavior change you can get widespread acceptance of. Nothing like the threat of bankruptcy to motivate employees to put a sticker on their insurance card.

