
Home » Posts tagged 'Mercer'
Tag Archives: Mercer
HERO Report: Wellness Industry Leaders Shockingly Admit that Wellness Is Bad for Morale

The question is: how do you help employees spend less and get healthier at the same time?
(March 14) This is the first in a series looking at the strengths and weaknesses of the HERO Outcomes Guidelines report, recently released by the Wellness Ignorati. One explanatory note: A comment accused us of insulting the Wellness Ignorati by calling them that. It is not an insult. It describes their brilliant strategy of ignoring facts and encouraging their supporters to do the same. We are very impressed by the disclipline with which they have executed this strategy, and will be providing many examples. However, if they prefer a different moniker to describe their strategy, they should just let us know.
We encourage everyone to pick up a copy of this report, the magnum opus of the Wellness Ignorati. Unlike the Ignorati, we are huge advocates of transparency and debate (which they call “bullying”). We want employers to see both sides and decide for themselves what makes sense, rather than spoon-feed them selected misinformation and pretend facts don’t exist.
The latter is the strategy of the Wellness Ignorati. Indeed, they earned their moniker by making the decision to consistently ignore inconvenient facts. (This is actually a smart move on their part, given that basically every fact about wellness is inconvenient for them.) For example, they just wrote 87 pages on wellness outcomes measurement without admitting our existence, even though we wrote the only book — an award-winning trade best-seller — on wellness outcomes measurement. Observing the blatant suppression of facts and the loss of credibility that comes with blatantly suppressing facts is just one of the many reasons to read this report. In total, their report provides a far more compelling argument against pry, poke, prod and punish programs than we ourselves have ever made, simply by bungling the (admittedly impossible) argument in favor of them.
There is too much fodder for us to deconstruct in one posting, so over the next several weeks we will highlight aspects of this report that we think are especially revealing about the sorry state of the wellness industry.
In terms of getting off to a good start, the Ignorati are right up there with Hillary Clinton, with their first self-immolation appearing on Page 10. Remember our mantra from Surviving Workplace Wellness: In wellness, you don’t have to challenge the data to invalidate it. You merely have to read the data. It will invalidate itself.
And sure enough…
Ironically, the first self-immolation is the direct result of that rarest of qualities among the Ignorati: integrity. We were shocked by the revelation that the Ignorati actually realize that employee morale and a company’s reputation both suffer when companies institute wellness programs – but here is the screenshot. Both morale and reputation are listed, as “tangential costs.”
Try telling a CEO that the morale of his workforce and his corporate reputation are “tangential” to his business. We ourselves run a company, and we would not list low morale as a “tangential cost.” Quite the opposite — our entire business depends on our employees’ intrinsic motivation to do the best job they can. If their morale suffers, our profit suffers. That’s why we would never institute a wellness program. The last thing we want to do is impact our morale in order to measure our employees’ body fat. Obviously, it is harder to hire and retain people if you value body fat measurement over job performance, and we are pleased to see the ignorati finally admit this.

Why, having now read this revelation in the ignoratis’ own words, that wellness is bad for morale, would any company still want to “do wellness”? Or as we say in Cracking Health Costs, “If you’re a general, would you rather have troops with high morale or troops with low cholesterol?”
The fact that employees hate wellness isn’t exactly a news flash. Anytime there is an article in the lay press, the public rails against wellness — or “bullies” the wellness industry, to use the term that the Ignorati use for people who disagree with them publicly. You don’t have to look far—just back to HuffPost on Wednesday. Or All Things Considered.
Obviously, if you have to bribe employees to do something (or fine them if they don’t), it’s because they don’t like it. If employees would rather sacrifice considerable sums of money than be pried, poked and prodded, they are sending you a message: “This is a stupid idea we want nothing to do with.”
The news flash is that this whole business of “making employees happy whether they like it or not,” as we say in Surviving Workplace Wellness is now acknowledged – by the Ignorati as a group — to be a charade.
HERO seems to have exhausted their integrity quota pretty quickly, because after that welcome and long-overdue and delightfully shocking admission, they slip back into character.

To get good answers, you must ask good questions. We do.
Specifically, in their listing of costs, they conveniently forgot a bunch of direct, indirect and “tangential” costs. Like consulting fees. Generally, the less competent and/or honest the consultants, the more they charge. (For instance, we can run an RFP for $40,000 or less, and measure outcomes for $15,000 or less — and do both to the standards of the esteemed and independent GE-Intel Validation Institute. Most other consultants can’t match either the price or the outcome.) We’re not calling any consulting firm incompetent or dishonest other than pointing to a few examples that speak for themselves, but it does seem more than coincidental that the consultants involved in this report have conveniently forgotten to include their own fees as a cost.
And what about the costs of overdiagnosis caused by overscreening far in excess of US Preventive Services Task Force guidelines? The cost of going to the doctor when you aren’t sick, against the overwhelming advice of the research community?
Still, we need to give credit where credit is due, so we must thank the Ignorati for acknowledging that wellness harms morale. It took even less time for this acknowledgement than for the tobacco companies to admit that smoking causes cancer.
Share this:

Stop the Presses: We Goofed!
When you are in the “countererrorism” business like we are, it’s important to have a zero tolerance for errors. Occasionally one slips through. In that case the important thing to do is to admit it, rather than fire the Attorney General and the Special Prosecutor and have your secretary erase the tape.
Vik and I wrote a posting for The Health Care Blog, the upshot of which was that the Affordable Care Act should no longer require insurers to cover adult checkups. Free checkups are ubiquitous in self-administered plans. On balance, our posting shows what grownups in health services research already know: they are worthless. Not completely satisfied with their innate worthlessness with a full subsidy, many employers — guided by benefits consultants — attach additional money to them: you are either fined for not getting one or else receive a bonus for getting one. Our proposed solution was/is quite simple: employers that attach bonuses or fines to physicial exams need to disclose that checkups are a waste of time and money. That simple disclosure requirement would end forced checkups.
It turns out, however, that adult checkups are not required by ACA. It was a complete benefits consulting urban legend and we fell for it. So we were wrong.
Here are the lessons from this.
First, if someone proves us wrong, we admit it. See? Admitting error is a concept that is lost on the wellness and benefits consulting industries. For example, after we pointed out that Mercer’s client British Petroleum got completely snookered by Mercer Staywell, the response of Mercer to BP wasn’t: “We apologize to for letting your vendor snooker you.” It was: “Let’s nominate this program for a Koop Award,” which naturally they won because both Mercer and Staywell are represented on the board of the group that gives out the award.
Second, the particular someone who proved us wrong, Chris Glason, did not “bully” us. He merely asked a tough question that invalidated a (minor) premise of our argument. However, when we do something quite similar, the people who are wrong (or lying) say we are “bullying” them. But all we did was ask 11 questions to clarify what someone already said — and offer him $1000 to answer the questions. Trust us: if Chris Glason had offered us $1000 to look it up and get back to him, we would have. (Instead we were rather dismissive, to put it mildly, for which we also publicly apologize.)
Third, our mistake was to assume that benefits consultants actually know something about, well, benefits consulting. We know they know nothing about wellness—Mercer and Milliman have both basically self-immolated by participating in the aforementioned Koop Award Committee and getting snookered four times by dishonest vendors. On two occasions the Committee was forced to backtrack as a result of our exposes, though they never admitted they got snookered. We kind of assumed that since benefits consultants don’t know anything about wellness, the only way they could stay in business was to actually know the first thing about benefits….and we listened to them.
Sidebar: a few benefits consultants are highly competent. We recommend the ones whom the Validation Institute (which is not connected with us but which we have a lot of respect for) has certified. (Don’t strain your eyes–no one from Mercer or Milliman appears on their listing.)
Fourth and most importantly, the answer doesn’t change: End “pry, poke, prod and punish” programs — especially the “prodding” part, now that even benefits consultants can see that prodding someone to go to the doctor when they aren’t sick is a complete waste of time and money.
“I made a mistake. I listened to the experts.”
— John F. Kennedy
Share this:

Ron Goetzel’s “Dumb and Dumber” Defense Deflects Latest Koop Award Ethical Scandal
By Al and Vik
Oh, the twists and turns as Ron “The Pretzel” Goetzel tries to wriggle out of all his ethical stumbles.
This time around, we thought we had nailed both him and his cabal handing out the ironically named C. Everett Koop Award to themselves and their friends based on made-up outcomes. Specifically, this time they gave their sponsor (Health Fitness Corporation, or HFC) an award based on data that was obviously made up, that no non-sponsor could have gotten away with submitting. This was the third such instance we’ve uncovered of a pattern of giving awards to sponsors for submitting invalid data while making sure that the award announcement contains no reference to the sponsorship. (There are probably others; we’ve only examined 3, which might explain why we’ve only found 3.)
How obviously was the data made up? Well, take a looksee at this slide, comparing participants to non-participants. This is the classic wellness ignorati ruse: pretending that non-motivated inactive non-participants can be used as a valid control for comparison to active, motivated participants. The wellness ignorati would have us believe that any healthcare spending “separation” between the two groups can be attributed to wellness programs, not to inherent differences in motivation between the two groups. Unfortunately for the ignorati, their own slide invalidates their own argument: in 2005, the label “Baseline Year” shows there was no program to participate in, and yet – as their own slide shows – participants (in blue) significantly underspent non-participants (in red) nonetheless. In Surviving Workplace Wellness, we call this “Wellness Meets Superman,” because the only way this could happen is for the earth to spin backwards.
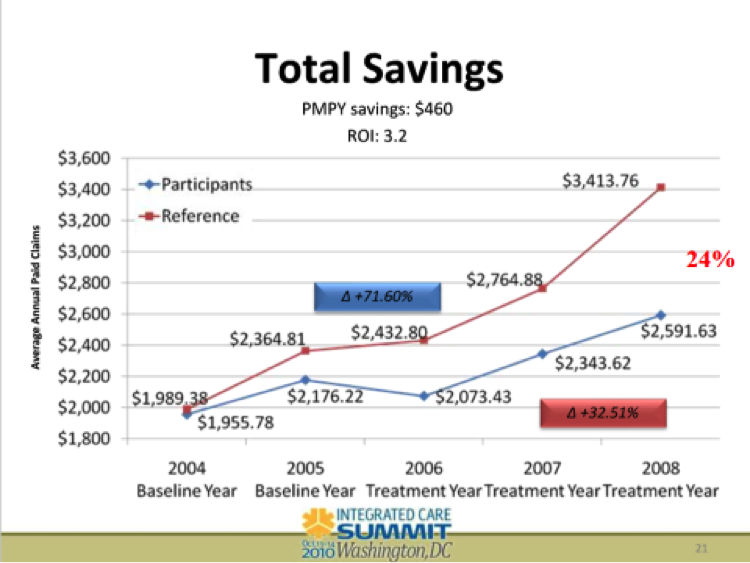
Given that the 2005 baseline label was in plain view, we just assumed that HFC did not indeed have a program in place for this customer (Eastman Chemical) in 2005, which is why they called 2005 a “Baseline Year” instead of a “Treatment Year.” Not actually having a program would logically explain why they said that didn’t have a program, and why they used that display or variations of it like the one below for 4 years with the exact same label. Presumably if they had had a program in 2005, someone at HFC would have noticed during those 4 years and relabeled it accordingly.
Originally we thought the Koop Award Committee let this invalidating mistake slide because HFC — and for that matter, Eastman Chemical — sponsor the awards they somehow usually win. But while trying to throw a bone to HFC, the Koop Award luminaries overlooked the profound implication that the year 2005 separation of would-be participants and non-participants self-invalidated essentially the entire wellness industry, meaning that is is an admission of guilt that the industry-standard methodology is made up.
 Goetzel the Pretzel to the rescue. He painstakingly explains away this prima facie invalidation. Apparently the year 2005 was “unfortunately mislabeled.” Note the pretzelesque use of the passive voice, like “the ballgame was rained out,” seemingly attributing this mislabeling to an act of either God or Kim-Jung-Un. He is claiming that instead of noticing this invalidator and letting this analysis slide by with a wink-and-a-nod to their sponsor, none of the alleged analytical luminaries on the Koop Committee noticed that the most important slide in the winning application was mislabeled — even though this slide is in plain view. We didn’t need Edward Snowden to hack into their system to blow up their scam. They once again proved our mantra that “in wellness you don’t need to challenge the data to invalidate it. You merely need to read the data. It will invalidate itself.”
Goetzel the Pretzel to the rescue. He painstakingly explains away this prima facie invalidation. Apparently the year 2005 was “unfortunately mislabeled.” Note the pretzelesque use of the passive voice, like “the ballgame was rained out,” seemingly attributing this mislabeling to an act of either God or Kim-Jung-Un. He is claiming that instead of noticing this invalidator and letting this analysis slide by with a wink-and-a-nod to their sponsor, none of the alleged analytical luminaries on the Koop Committee noticed that the most important slide in the winning application was mislabeled — even though this slide is in plain view. We didn’t need Edward Snowden to hack into their system to blow up their scam. They once again proved our mantra that “in wellness you don’t need to challenge the data to invalidate it. You merely need to read the data. It will invalidate itself.”
We call this the “Dumb and Dumber” defense. Given two choices, Goetzel the Pretzel would much prefer claiming sheer stupidity on the part of himself, his fellow Koop Award committee members like Staywell’s David Anderson and Wellsteps’ Steve Aldana, and his sponsor HFC, rather than admit the industry’s methodology is a scam and that they’ve been lying to us all these years to protect their incomes.
Still, the Dumb-and-Dumber defense is a tough sell. You don’t need Sherlock Holmes, Hercule Poirot or even Inspector Clouseau to detect a few holes in the Pretzel’s twisted logic:
- How could no one – no member of the Koop Award Committee or employee of Health Fitness Corporation (which used this as its “money slide” for years) – have noticed this until we pointed it out for the third time (the first two times not being as visible to the public)?
- In early 2012, this slide was reproduced–with the permission of Health Fitness Corporation–right on p. 85 of Why Nobody Believes the Numbers, with the entire explanation of its hilarious impossibility. We know Mr. Goetzel read this book, because he copied material out of it before the publisher, John Wiley & Sons, made him stop. So we are curious as to why it has taken until now for him to notice this “unfortunate mislabeling.” Hmm…would the fact that it was just exposed to the world in Health Affairs have anything to do with this sudden epiphany? We’re just sayin’…
- If indeed it was just an “unfortunate mislabeling,” how come HFC has now expunged all references to this previously highlighted slide from their website, rather than simply change the label?
As regards the third point, we would recommend that next time Mr. Goetzel invokes the Dumb-and-Dumber defense, he coordinate his spin with his sponsor.
But let’s not overlook the biggest point: the entire Koop Committee – including “numbers guys” like Milliman’s Bruce Pyenson and Mercer’s Dan Gold — is apparently incapable of reading a simple outcomes slide, as they’ve proven over and over.
So, as a goodwill gesture, we will offer a 50% discount to all Koop Committee members for the Critical Outcomes Report Analysis course and certification. This course will help these committee members learn how to avoid the embarrassing mistakes they consistently otherwise make and (assuming they institute conflict-of-interest rules as well to require disclosure of sponsorships in award announcements) perhaps increase the odds that worthy candidates win their awards for a change.
Share this:

Milliman Magic Saves North Carolina More Medicaid Money Than Was Actually Spent
Milliman, Community Care of North Carolina
Short Summary of Intervention:
Increase payments to providers and add EMRs and add case managers in the hopes of reducing admissions and emergency room expenses
Links to and List of Materials Being Reviewed:
- Milliman Cost Savings Report
- Questioning the Widely Publicized Savings Reported for North Carolina Medicaid



Summary of key figures and outcomes:
- $177-million savings in 2007 in children’s admissions alone, increasing in the years after that
- Increase in costs of program more than offset by admissions reduction
Questions for Community Care of North Carolina:
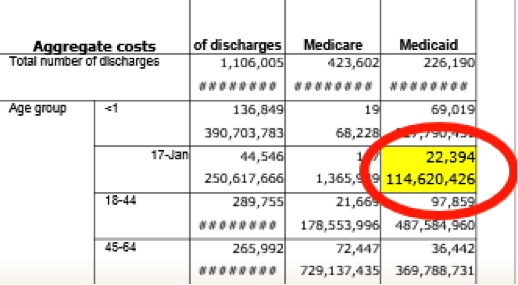
The CCNC website says CCNC is “saving money” and yet the federal government data above notes that North Carolina Medicaid’s costs are between 24% and 40% higher than the costs in surrounding states. How is this “saving money”?
ANS: Refused to answer
North Carolina has suffered cost overruns amounting to more than a billion dollars just since CCNC became the provider for almost all non-disabled adults and children in the state. How is that track record consistent with “saving money”?
ANS: Refused to answer
Why did you hire consultants — and pay them more taxpayer money than any other consultants had ever been paid to do this work — who had never done this type of analysis before and didn’t even realize that the answers were already online?
ANS: Refused to answer
Questions for Milliman:
How is it possible to save at least $177,000,000/year starting in 2007 in children’s admissions when the government’s own data collected expressly for the purpose of studies like these shows you only spent $114,000,000 in 2006?
ANS: Refused to answer
Your defense has been that 2006 was not the baseline. However, the years prior to 2006 all show spending figures lower than $114,000,000. So which year was the baseline?
ANS: Refused to answer
You have also said that there is no baseline period. Can you point us to any other study in any reputable journal which did not have a baseline period?
ANS: Refused to answer
Why did you suppress all the government data above that completely contradicted your findings, or did you not know the government collected this data both on comparative per capita costs and on admissions by age group and payer?
ANS: Refused to answer
If you did not know about this online data, shouldn’t you be changing your conclusions and/or returning North Carolina taxpayers their money?
ANS: Refused to answer
If you thought this authoritative government data showing the opposite was irrelevant or wrong, could you explain why?
ANS: Refused to answer
Were you aware that Mercer’s previous study for North Carolina was also thoroughly discredited for not using that government data and thereby coming up with an impossible answer (the study has quietly been removed from the Community Care of North Carolina website as a result)?
ANS: Refused to answer
If surrounding states have similar Medicaid programs and most North Carolina children were already in CCNC, why not just take advantage of that “natural control” and compare the state as a whole to other states, especially because the federal data mentioned above had already been collected for all those states?
ANS: Refused to answer
In your Letter to the Editor following publication of the above article questioning your savings, which consisted of four questions about the savings calculation, why you didn’t answer any of the four questions the article asked?
ANS: Refused to answer
The very first page of your report says the decline in admissions more than offset the increases in other categories, thus netting out to the massive savings you calculated. Yet after it was shown that admissions did not decline at all, you said in your Letter to the Editor that the decline came from “categories other than admissions.” Which is it – admissions accounted for more than 100% of the net savings, offset by other categories, or other categories accounted for all the savings?
ANS: Refused to answer
Page 19 of your report says “other Milliman consultants may hold different views.” If members of your own organization wouldn’t agree with you, why should others agree with you when you suppressed data, contradicted yourself, and found mathematically impossible savings?
ANS: Refused to answer
Admission rates in the specific disease categories CCNC was focused on — asthma and diabetes — underperformed surrounding states. In diabetes admissions actually increased on an absolute basis. Where did the savings come from if not from the targeted conditions?
ANS: Refused to answer
Share this:

Is Mercer Cooking Staywell’s Books At British Petroleum?
Staywell, Mercer
Short Summary of Intervention:
Comprehensive wellness program offered to all American employees of British Petroleum. Staywell was the vendor. Mercer was hired by British Petroleum to validate the savings claimed by Staywell.
Materials Being Reviewed
- Staywell and Mercer Analysis of British Petroleum Program
- The Health Care Blog Review of British Petroleum Wellness Program
Summary of key figures and outcomes:
No visuals were provided. A review of the articles is recommended.
Questions for Staywell and Mercer
You claimed that spending would have increased by 10.5% instead of 7% across the entire company, absent the wellness program. Since only 1139 people reduced their risk factors (not including non-participants and dropouts whose risk factors might have increased), are you saying that by reducing a risk factor, those 1139 people were responsible for the entire difference in trend for the 62,000 employees and dependents versus the original trend you projected?
ANS: Refused to answer
The savings you are claiming works out to about $17,000 for each person whose risk factors declined, almost the equivalent of avoiding one heart attack for each person who reduced a risk factor. Are you suggesting that most of those 1139 would have had heart attacks otherwise, even though fewer than 200 American BP employees had a heart attack the previous year?
Note to Staywell’s and Mercer’s actuaries: if costs decline $17,000 every time someone reduces a risk factor and your spending is about a third of that level, you can wipe out your healthcare bill by getting a third of your employees to reduce a risk factor.
ANS: Refused to answer
How does $17,000 in savings for BP employee reducing a risk factor reconcile with Staywell’s own website claiming only $100 in savings for each person reducing a risk factor in a multi-employer study?
ANS: Refused to answer
How does this unprecedented savings reconcile with the PepsiCo findings, published in a leading journal (Health Affairs) by leading researchers (RAND), that concluded applying approximately the same interventions to PepsiCo’s workforce using the same consulting firm (Mercer) actually lost money?
ANS: Refused to answer
Did Mercer notice the discrepancy between Staywell’s alleged results and PepsiCo’s (and also Staywell’s own website) and inform British Petroleum of it, since Mercer’s job was to validate this program on behalf of British Petroleum and ensure that the savings were accurate?
ANS: Refused to answer
Since a wellness program can only reduce wellness-sensitive medical events, how come you elected not to disclose the rate of wellness-sensitive medical events across the entire population before and after the program?
ANS: Refused to answer
Did you inform British Petroleum that there was an article on The Health Care Blog about their program that reached the opposite conclusion you reached?
ANS: Refused to answer
Staywell employees Jessica Grossmeier (who authored the journal article) and Paul Terry (Chief Science Officer) were asked privately and by many of the people who posted comments to rebut The Health Care Blog and declined. Wouldn’t it have been a useful discussion to explain to readers how British Petroleum could have saved more than 100 times what you yourself said was possible?
ANS: Refused to answer
Share this:
More Milliman Magic From North Carolina
Milliman, Community Care of North Carolina
Short Summary of Intervention:
Increase payments to providers and add EMRs and add case managers in the hopes of reducing admissions and emergency room expenses
Links to and List of Materials Being Reviewed
- Milliman Cost Savings Report
- Questioning the Widely Publicized Savings Reported for North Carolina Medicaid


Summary of key figures and outcomes:
$177-million savings in 2007 in children’s admissions alone, increasing in the years after that
Increase in costs of program more than offset by admissions reduction
Questions for Community Care of North Carolina:
The CCNC website says CCNC is “saving money” and yet the federal government data above notes that North Carolina Medicaid’s costs are between 24% and 40% higher than the costs in surrounding states. How is this “saving money”?
North Carolina has suffered cost overruns amounting to more than a billion dollars just since CCNC became the provider for almost all non-disabled adults and children in the state. How is that track record consistent with “saving money”?
Why did you hire consultants — and pay them more taxpayer money than any other consultants had ever been paid to do this work — who had never done this type of analysis before and didn’t even realize that the answers were already online?
Questions for Milliman
How is it possible to save at least $177,000,000/year starting in 2007 in children’s admissions when the government’s own data collected expressly for the purpose of studies like these shows you only spent $114,000,000 in 2006?
Your defense has been that 2006 was not the baseline. However, the years prior to 2006 all show spending figures lower than $114,000,000. So which year was the baseline?
You have also said that there is no baseline period. This strikes us as curious but we could be wrong: Can you point us to any other study in any reputable journal which did not have a baseline period?
Why did you suppress all the government data above that completely contradicted your findings, or did you not know the government collected this data both on comparative per capita costs and on admissions by age group and payer?
If you did not know about this online data, shouldn’t you be changing your conclusions and/or returning North Carolina taxpayers their money?
If you suppressed the data because you thought it was irrelevant, wouldn’t it have been more ethical to acknowledge the existence of the authoritative government data, but then describe why the federal government data didn’t apply and let the reader decide whether it was relevant?
Given that Mercer’s previous study for North Carolina was thoroughly discredited for not using that government data and thereby coming up with an impossible answer (the study has quietly been removed from the Community Care of North Carolina website as a result), wouldn’t it have been wise not to make that same mistake again?
If surrounding states have similar Medicaid programs and most North Carolina children were already in CCNC, why not just take advantage of that “natural control” and compare the state as a whole to other states, especially because the federal data mentioned above had already been collected for all those states?
In your Letter to the Editor following publication of the above article questioning your savings, which consisted of four questions about the savings calculation, why you didn’t answer any of the four questions the article asked?
The very first page of your report says the decline in admissions more than offset the increases in other categories, thus netting out to the massive savings you calculated. Yet after it was shown that admissions did not decline at all, you said in your Letter to the Editor that the decline came from “categories other than admissions.” Which is it – admissions accounted for more than 100% of the net savings, offset by other categories, or other categories accounted for all the savings?
Page 19 of your report says “other Milliman consultants may hold different views.” If members of your own organization wouldn’t agree with you, why should others agree with you when you suppressed data, contradicted yourself, and found mathematically impossible savings?
Admission rates in the specific disease categories CCNC was focused on — asthma and diabetes — underperformed surrounding states. In diabetes admissions actually increasing on an absolute basis. Didn’t you feel this might be a red flag to suggest that the huge savings your model was showing you might not be valid?
Share this:

Mercer Says “Choice of Trend” Drives Savings Estimates
Mercer
Short Summary of Intervention as described by company:
Mercer Health AdvantageSM – Mercer Health Advantage (MHA) allows self-funded employers to enroll their employees in new medical plans starting January 1, 2013. These programs are designed to save employers 5% or more of medical plan cost with the same plan design they have in place today. The savings come from select networks with providers chosen for their quality and cost effectiveness. Employers also gain access to dedicated MHA clinical care management with ongoing oversight and audit by a team of Mercer clinicians. Mercer plans to offer MHA to smaller self-funded employers in 2014. Self-insured clients with Aetna need 1,000 employees, Anthem-1,500 employees or greater on WGS or NASCO claims platform and UHC must have 3,000 employees in the National Accounts segment.
Materials Being Reviewed
All publicly available Mercer outcomes reports and related materials, plus Mercer Health Advantage
Related materials:
- Georgia Medicaid
- North Carolina Outcomes Excerpts below
- Staywell and British Petroleum
Summary of key figures and outcomes:
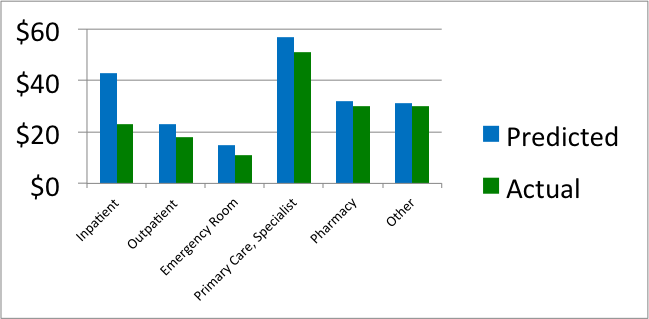
Comparison of actual vs. predicted spending per North Carolina Medicaid member per month in medical home, by category of service
Predicted vs. actual by age grouping for North Carolina Medicaid enrollees in medical home
 Questions for Mercer
Questions for Mercer
I: Mercer Health Advantage
Since most employers spend less than 5% of their total budget on disease management-sensitive events, how is it possible to save 5% through a disease management program even by eliminating every event with no increase in preventive expenses?
ANS: Refused to answer
If the state of Georgia were able to save 19% through APS disease management, which according to your own reconciliation APS is able to do, shouldn’t you be advising clients to use APS or another vendor instead of yourselves?
ANS: Refused to answer
If you are being retained to help a client find the best disease management solution, wouldn’t offering your own such solution create a conflict of interest?
ANS: Refused to answer
How have you determined the quality and cost-effectiveness of physicians that you “choose” for this network?
ANS: Refused to answer
II: Mercer North Carolina Patient-Centered Medical Home Analysis
The first North Carolina chart shows savings in every category. How is it possible to save money in all categories? Doesn’t some component of spending have to go up to make everything else come down? Or, as the outcomes measurement textbook says: “If you insulate your house, you’ll save money on heat, but not on insulation.”
ANS: Refused to answer
Is it possible that the reason savings appeared in all categories is that you simply chose to project a high trend, so that you could show more savings against that trend, or as you’ve said in the past: ““We can conclude…that the choice of trend has a large impact on estimates of financial savings”?
ANS: Refused to answer
If medical homes save money through more primary care reducing the need for specialist visits, why combine both categories when reporting savings?
ANS: Refused to answer
Inpatient spending fell by more than 50%, which implies that non-birth-event admissions would have fallen by more than 70%. How does this reconcile with the official government admissions data, which shows no change in admissions?
ANS: Refused to answer
There was no noticeable decline in North Carolina in the official government list of primary care-sensitive admissions during the period you analyzed. How do you reconcile that data with your own data showing massive admissions reduction?
ANS: Refused to answer
The second North Carolina chart shows that per-member per-month expenses in children under 1 year of age declined more than 50%. Since there is essentially no common chronic disease in this age group, where did the savings come from?
ANS: Refused to answer
The largest expenditure in this age group is in neonates. How does your data reconcile with the government data showing no change in neonatal admissions?
ANS: Refused to answer
How were you able to show such massive savings for this age group in your medical home analysis when this age group wasn’t eligible for the medical home?
ANS: Refused to answer
III: Mercer Georgia Analysis
Assuming that disease management-sensitive medical events account for roughly 8% of spending in a Medicaid population, how is it possible to save 19% through a disease management program?
ANS: Refused to answer
How do you reconcile your conclusion that the APS disease management program saved 19%, when an FBI investigation found that APS had largely failed to perform its disease management services?
ANS: Refused to answer
IV: Staywell and British Petroleum
Did you caution British Petroleum that the savings you validated for them was at least 100 times the savings that Staywell itself claims is possible?
ANS: Refused to answer
Did you question Staywell about how they were able to outperform their benchmark by 100-fold?
ANS: Refused to answer
Why didn’t you or Staywell provide your viewpoint when requested to, following the observations on The Health Care Blog that these savings were mathematically impossible?
ANS: Refused to answer
V: Mercer Qualifications to Do Outcomes Analysis
It appears that no one at Mercer has ever achieved Advanced or even Standard Certification in Critical Outcomes Report Analysis, either through DMPC or one for the Validation Institute that is specifically geared to benefits consultants. Has any Mercer consultant taken either course and failed, or has no one at Mercer ever taken either course?
ANS: Refused to answer
Assuming the mistakes highlighted above are innocent miscalculations and not purposeful deceptions – and with senior consultant hourly billing rates well in excess of $500/hour – don’t you think it would be a good idea to become qualified in analyzing outcomes reports and reconciliation methodologies that you are being paid to analyze?
ANS: Refused to answer
Is there another course in outcomes analysis that we are unaware of that your consultants have taken, and if so, how did they still make all the mistakes above?
ANS: Refused to answer
Share this:

Health Fitness Corp wins a Koop award for curing non-existent cancers in Nebraska
C. Everett Koop National Health Award Committee,
Wellness Council of America and Health Fitness Corp.
Short Summary of Award:
The C. Everett Koop award committee’s mission is:
“…to seek out, evaluate, promote and distribute programs with demonstrated effectiveness in influencing personal health habits and the cost effective use of health care services. These programs have the objectives of
- Providing appropriate quality care
- Sharply reducing the alarming rate of health care inflation, by holding down unnecessary expenditures.”
Materials Being Reviewed:
The brochure in question describing the Nebraska program is downloadable from the WELCOA website.
Case Study of Award Winner for 2012: Health Fitness Corporation and Nebraska
Summary of key figures and outcomes:
Alleged cancer outcomes include the following:
Risk reduction outcomes include the following:

Questions for C. Everett Koop Award Committee:
I: Alleged Cancer Outcomes
Were you troubled by the program sponsors’ decision to waive all age-related colon cancer screening guidelines established by the government, and send out 140,000 flyers, at taxpayer expense, featuring a beautiful woman much too young to have a screening colonoscopy?
ANS: Refused to answer
How come, when the program reported that 514 of the 5000 (or fewer) people screened had colon cancer (in addition to the ones who would have been screened anyway), none of the Committee members with health informatics backgrounds from Truven Health Analytics and Mercer and Milliman (and from Wellsteps and Staywell, both of whose programs are also highlighted) were concerned that this alleged 11% colon cancer rate was at least 100 times greater than Love Canal’s?
ANS: Refused to answer
When Health Fitness Corporation admitted lying and reversed their story from making “life saving, cost-saving catches” of “early stage [colon] cancer” to revealing that those 514 people didn’t have cancer, why did the Koop Committee re-endorse what would appear to be outright data falsification, instead of rescinding the award?
ANS: Refused to answer
Even if the committee is allowing Health Fitness Corporation to keep its award and not even apologize, why does this claim of “life-saving, cost-saving catches” still appear on the WELCOA website even though the lie has been admitted?
ANS: Refused to answer
Wouldn’t the fact that the perpetrator of this acknowledged lie is also a sponsor of this Koop award that its own customers have won three times (including this incident) create the perception of a conflict of interest?

ANS: Refused to answer
Does anyone on the Committee think if Dr. Koop were still alive that he would endorse your position on data falsification of cancer victims?
ANS: Refused to answer
WELCOA’s website said it was founded by someone who appears to be the inventor of the self-serve all-you-can-eat restaurant. Despite his well-deserved reputation for integrity, did he endorse data falsification of cancer victims even after the perpetrators admitted it?

ANS: Refused to answer (but did change the spelling)
II: Risk Reduction Outcomes
How do you reconcile the claimed savings figure exceeding $4-million with your own chart above showing that only 161 active participants (3.1%) reduced a risk factor? (That chart of course doesn’t include dropouts and non-participants, whose risk factors may have increased.)
ANS: Refused to answer
Dividing the total savings by 161 yields more than $20,000/person in savings. Wouldn’t that $20,000+ for each risk factor avoided imply that all 161 would have had a heart attack even though the entire eligible population only had about 30 heart attacks the previous year, while the participating population would have had about 7?
ANS: Refused to answer
How do you reconcile your statement that 40% of the population had previously undiagnosed high blood pressure or high cholesterol with your other statement that “the total number of prescription scripts [sic] filled within the Wellness Plan reduced [sic] 3% last year,” despite your reducing or waiving the copays? Shouldn’t prescriptions have gone up, if indeed 40% more people were at risk?
ANS: Refused to answer
How can you attribute the 3% reduction in prescriptions to “improved lifestyles” with the fact that your own graph shows only 161 people improved their lifestyles enough to reduce a risk factor? What happened to the thousands who were diagnosed but were neither medicated nor improved their lifestyles?
ANS: Refused to answer
How do you reconcile that same finding – that 40% had high blood pressure or cholesterol — with that same graph, showing that almost three-quarters of the population was low-risk?
ANS: Refused to answer
How do you reconcile the brochure’s claim that the “majority of employees touted how the program has improved their lives” with the brochure’s own admission that only a minority of employees (42%) even bothered to be screened once and only 25% twice despite the four-figure financial incentive?
ANS: Refused to answer
Follow-up response
Not-for-attribution response received August 1, stating that the reason the Committee let them keep their award was not because were a sponsor but rather because they did not make the life-saving claim on their application. (They did make all the other invalid claims.) Because they didn’t make the claim on the application, they are not in violation of the Committee’s ethical standards by making it in other venues.
Our reaction:
So it is OK if a ballplayer admits using steroids as long as he didn’t happen to test positive?
Follow-Up Response
September 2014: Nebraska listed as a “best practice program” by Ron Goetzel
Our Reaction:
Doesn’t this listing contradict your initial excuse — that you forgot to ask them about whether they made up their cancer statistics during your due diligence — because now you know about that lie and all the other lies in their outcomes measurement…and yet you still call them a best-practice program?

