
Home » Uncategorized (Page 10)
Category Archives: Uncategorized

Life imitates The Price We Pay
If there’s one thing you learn from Marty Makary’s blockbuster expose The Price We Pay (other than Quizzify being a great vendor, on page 226), it’s not to get a peripheral vascular screen at a community center.
Here are his exact words from his trip to a community center hosting a screening session for peripheral vascular disease:
The person from the cardiology group was conducting a test that measures how the blood flow in the legs compares to the blood flow in the arms. The rationale: Something might be wrong if the blood pressure is lower in the legs. It could be caused by a narrowing of the arteries, a plaque that slows blood flow. It might warrant further investigation.
There’s just one problem with that notion: This test should not be performed unless a patient has serious symptoms, like crippling leg pain. For anyone else, it’s likely to lead to medical care they don’t need, which can be expensive and dangerous. That’s exactly why independent medical experts do not recommend the type of peripheral vascular screening I witnessed that day.
So, thanks to the chronic shortage of other subject matter for these periodic blogs now that wellness vendors have finally learned not to brag publicly about their stupidity, imagine my glee when a brochure from Life Line Screening arrived in the mail last week urging me to: get peripheral vascular screening at a community center.
Not only that, but my special “priority code” meant I “qualified” for a large, exclusive, discount (“Only $149”). I was very pleased to hear that — just like achieving Mosaic on JetBlue, Titanium Ambassador in Marriott, and something like Executive Platinum Emerald Diamond Palladium Plutonium Selenium Sodium Fluoride on American — I had also achieved “Status” with Life Line.
Needless to say I wanted to brag about this achievement to all my friends-and-relations who also got this mailing. But my ego took a hit when I learned that apparently they too received high-priority codes and qualified for this exact same exclusive discount. Trying to figure out what we all had in common to earn this special treatment, we concluded that this it was being offered — exclusively — to people who are comprised of protoplasm.
In addition to the peripheral vascular disease screening, rated “D” by the US Preventive Services Task Force in my 40-64-year-old group, they are offering the following additional “vital screenings,” with the USPSTF rating in parentheses:
- Abdominal aortic aneurysm screening (D for nonsmokers under 65)
- Heart rhythm screening (I rating)
- Osteoporosis (I rating)
- Carotid artery screening (D rating)

For those uninitiated in USPSTF screening ratings, “D” means “don’t screen for this,” because of the overwhelming likelihood that positives will be false.
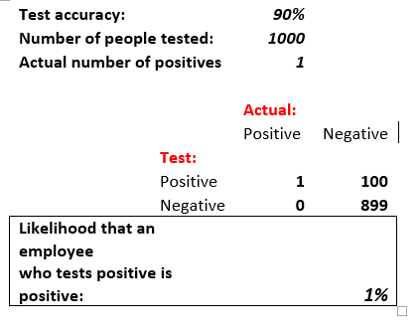
How overwhelming is this likelihood? Let’s take an example. Suppose you perform a test that’s 90% accurate to hunt for a previously undetected, symptomless, disease in 1000 people. Suppose further that about 1 in 1000 adults 40 to 64 has this undetected disease. A 90% accurate test is also 10% inaccurate. So, including the one person who actually has the disease, about 100 of the other 999 will test positive — despite being disease-free.
Those 100 are going to be totally stressed out for no reason, probably follow up with more tests, and possibly even get surgery. Here is the math:
Continuing with my USPSTF grading lesson for Life Line, “I” means “Incomplete,” not enough data for a recommendation. I don’t have to tell you what “A” and “B” mean because those ratings don’t apply to any of Life Line’s screens. That’s right. None of Life Line’s tests are recommended by the specific entity charged with recommending tests.
Needless to say, I couldn’t pass up the opportunity to call these Very Stable Geniuses. My call was answered by a Life Line employee who announced: “My name is XXXX. I’m going to be your Preventative Healthcare Advisor.” When I asked if these tests had an A Rating from from the US Preventive Services Task Force, she replied: “Very very very true. Also an A-Plus rating from the Better Business Bureau.”
She also assured me I could keep my clothes on, which I know the staff and guests of the Wellesley Community Center will appreciate.
The benefits of screening

Hmmm. Let’s look at each of these five claims in turn.
- “Early detection.” Check. Detection of more false positives than every wellness vendor except possibly Interactive Health, which specializes in them. (See “Interactive Health gives clueless wellness vendors a bad name.“)
- “Prevention of disease progression.” Screening might possibly detect something but it doesn’t prevent anything. Here’s what might prevent something: spending that $149 on a new pair of sneakers and running in the opposite direction of the Wellesley Community Center.
- “Peace of mind.” Try telling that to all the people who are getting false positives.
- “Savings with more affordable screenings.” I called my Preventative Healthcare Advisor to ask about that one. Turns out, as noted below, I can practically retire off these savings.
- “Control, no insurance required” ? “Required” is synonymous with “coverage” in this case. Just like “true” was synonymous with “false” about the USPSTF A ratings.
So…doctors don’t do these screens, insurance doesn’t cover them, and yet somehow, somehow, these screens are… “vital“? Time for another call to my preventative healthcare adviser to find out why, if these tests are so vital, doctors don’t do them. She explained that:
- Doctors will only do these tests for: “a reason” (shame on doctors!)
- But by then it might be “too late.”
- Doctors don’t do these tests routinely because they cost “$5000 to $8000,” instead of $149. That’s why the brochure lists “savings” as a benefit. You could save thousands right now by doing these screenings! Likewise, think of all the money you’re saving this month alone by not living in a $5000/month apartment.
- “Insurance companies are all about the money. They try to control our lives. That’s why they won’t pay for these tests.” (There is actually an element of truth to this one. Insurance companies are all about the money. Not unlike Life Line, which is clearly in business for their health, since they aren’t in it for ours.)
Postscript: I did check in with a primary care physician, who observed that she’s heard of doctors doing tests without “a reason.” But advertising that they do tests for no reason? That was news to her. She said they could lose their license. I pointed out that wellness vendors don’t need licenses, or for that matter even GEDs. Just the willingness to check their ethics at the door of the Wellesley Community Center. Plus a soupcon of protoplasm.
Share this:


Last call for Thursday’s “The cure for surprise billing” webinar
Dear They Said What Nation,
Besides the minor points that your employees’ or dependents’ odds of getting one of these surprise bills are 10 times the odds of having a heart attack or diabetes hospitalization* and that unlike the latter, these bills are utterly avoidable, here are three major reasons to sign up for this webinar:
- The 1500th registrant receives a $100 Amazon gift card from the Validation Institute, assuming they attend.
- You do NOT have to “attend” the webinar to experience it. Registrants will be given the recording. But you do have to register here.
- The way to be certain this is a valuable webinar that will result in easy, major, immediate, behavior change for any employer that implements our elegant solution is that no Koop Award-winning wellness vendor has registered for it — despite the fact that Whole Foods would redeem the gift card for almost all the broccoli you can eat.
A handful of other wellness vendors have signed up. We salute them.

- Aduro
- Health Advocate
- It Starts with Me
- Maestro Health
- US Preventive Medicine
And a special Honorable Mention to Wellable for posting the Reader’s Digest version of the webinar right here.
PS If you are a wellness vendor specifically, and I missed you while scanning the ridiculously long list of attendees, ping me and I’ll add you. Or sign up now and I’ll add you.
*OK, here is the calculation. The lower bound of these odds on any ER visit or admission is about 1-in-5 for any in-network facility according to the Kaiser Family Foundation. Others pace the odds at twice that, but we’ll go with the more conservative estimate. Your covered population incurs about 240 ER visits and admissions in total. 20% of 240 is: 48 per 1000. Whereas the number of covered people who will get a heart attack or have a diabetes event is 2 per 1000.
Oh, did I say surprise bills were ten times as likely? That would make them 24 times as likely.
And yet, unlike heart attacks and diabetes, totally avoidable…
Share this:


Care to guess the odds of a surprise medical bill for an ER visit?
According to a study published in JAMA Internal Medicine, an employee’s odds of getting a surprise medical bill for an ER visit or a hospital stay exceed 40%!
Well, you might say, serves ’em right for not staying in-network.
Wrong. This study looked only at in-network visits and admissions. Thing is, in-network facilities are often staffed with out-of-network providers. I know this firsthand — I’m in a private equity fund that’s making a killing by rolling up provider practices in local markets and keeping them out of network. It’s illegal for provider practices to collude to stay out of network, but it is perfectly legal for them to merge and make a practice-wide decision to stay out of network.
So, wellness vendors and consultants, here are two opportunities you can’t refuse, that are both central to your business strategy:
- Actually do something useful for employees, as opposed to your usual scripted diatribes. Newsflash: employees already know they need to quit smoking and eat broccoli. But they don’t know how to avoid these bills.
- Prevent me from making money.
Also, this is the one thing that could bankrupt them that is totally avoidable. And yet your financial wellness program doesn’t cover it.
Fortunately, if you can spare one short hour on October 31 (which you will get back 38 hours later, when the time changes), you can learn how your employees can avoid these bills. All it takes is a little sticker to put on an insurance card and teaching employees to use their card, rather than sign whatever is put in front of them and/or say: “Same as last year” when they ask you if your insurance information has changed.
The all-star cast of this webinar includes David Contorno, Brian Klepper, Marty Makary, and Marilyn Bartlett. You can register here.
PS If you can’t make the time because of open enrollment, you’ll have access to the recording.
Share this:


WTF! Introducing the wellness industry’s Wishful Thinking Factor

Finally! A valid way to measure wellness outcomes that requires only a calculator, a triple-digit IQ, and complete suspension of disbelief! Introducing the Wishful Thinking Factor, or WTF. Those of you accustomed to reviewing wellness vendor outcomes may think those initials stand for something else…and we will indeed use those initials in their more common context at the end of this posting.
By contrast, this WTF is defined as:
Dollars claimed as savings/percent improvement in risk factors.
The elegance of the WTF is exceeded only by its widespread acceptance. WTF is already the wellness industry’s preferred analysis, so I am merely confirming that we agree. The only difference between my WTF calculation and theirs is they don’t actually put the numerator and denominator on the same page.
Meaning, they don’t actually announce: “Here’s our huge savings generated by our trivial risk reduction…wait…this is impossible…WTF???”
That’s because then it would be perfectly obvious that they are fabricating the savings. Instead they put “dollars saved” on one page and the improvement in risk factors on another page, way far away — and hope nobody compares them. (Interactive Health is the most stable genius example of that, as we’ll see below.)
What is the real causal relationship between risk reduction and savings?
A distressingly relevant joke circulated among us rip-roaringly hilarious faculty back when I taught in the Harvard economics department. A chemist, physicist and economist are stranded on a desert island with only a can of beans. To open it, the physicist suggests dropping it off a cliff, so that it will open upon impact. The chemist points out that would splatter the contents, and suggests instead that they put the can in a fire, and once the can gets hot enough, it will melt. The physicist points out that the beans would all burn up in the fire. At an impasse, they turn to the economist and ask what he would do.
The economist replies: “Assume a can opener.”
In keeping with that spirit, we will make six (count ’em, 6) equally generous assumptions for determining the true WTF:
- Every wellness-sensitive medical admission or ER visit is a direct function of the risk that the wellness vendor measures in a population. In other words, social determinants of health and genetics have nothing to do with the likelihood of a heart attack or diabetes event
- Even the dumbest wellness vendors know how to measure risk (following their five days of training in medicine)
- Employees never cheat to improve their biometric scores and never lie on their risk assessments
- Dropouts and non-participants would improve in risk at the same rate as participants do, so the fact that they don’t participate doesn’t change the overall risk reduction in the population
- No lag time between risk reduction and event avoidance
- No false positives, no added lab tests, drugs, doctor visits or anything else that might possibly increase utilization and cost of outpatient care in order to reduce inpatient utilization — which of course is the opposite of what the wellness trade association readily admits to:

Using those generous assumptions, measured wellness-sensitive medical admissions (WMSAs), and the total cost of those events, would decline at the same rate as measured risk declines. According to the Health Enhancement Research Organization, WSMAs comprise no more than $100 PEPY in a commercially insured population. So every 1% decline in risk yields a spending decline of $1.
Relaxing the assumptions above would likely reveal that this WTF is also overstated, but it has the advantage of consensus among the 60+ experts who contributed to the HERO outcomes guidelines measurement tool, so we’ll call this the Gold Standard, to which other WTFs are compared.
Now let’s make a little list of the WTFs compiled by the industry’s very stable geniuses, in their great and unmatched wisdom. Naturally, in that category, the first to come to mind are Interactive Health and Ron Goetzel.
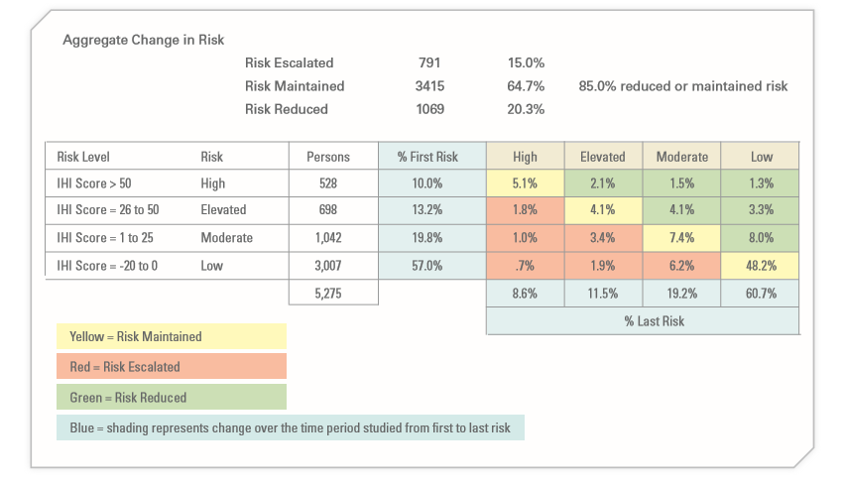
Let’s start with Interactive Health. Excluding dropouts and non-participants, they claimed a 5.3% risk reduction (20.3% reduced risk while 15% increased them). So they saved a maximum, assuming the six assumptions above, $5.30 PEPY:
The claimed savings was:

Averaging those claims yields $804, for a WTF of 151.
As a side note, allocating that $804 in savings across the 5.3% who actually did see a decline in risk factors yields over $15,000 per risk factor reduced. No mean feat when you figure that the average person only incurs about $6000 in employer spending. That was enough to get them in the Wall Street Journal
A second example (and there are many more) is the Koop Award given to Health Fitness Corporation for lying about saving the lives of cancer victims who never had cancer. The coverup of that fabrication was the lead story about Nebraska, along with whether Ron Goetzel had committed an actual crime, as opposed to simply snookering the rather gullible state, whose reaction when they found out is best described as Human Resources-meets-Stockholm Syndrome.
Mr. Goetzel defended his actions by saying that lying about saving the lives of cancer victims was overlooked by the awards committee, and what really earned Nebraska the award was saving $4.2 million by reducing 186 risk factors. Let’s calculate the WTF from that.

the absolute reduction in risk was 0.17 (1.72 to 1.55) on a scale of 7, or roughly 2.4%. That represents about 180 people out of 5199 reducing a risk factor. (Of course, the remaining 15,000 of the 20,000+ state employees dropped out and/or wanted nothing to do with this program, but that’s a different story. So much winning!)
And yet somehow, despite only 180 people claiming to reduce a risk factor, the program saved $4.2-million, or $807 apiece for the total 5199 people. That yields a WTF of 336.
Speaking of Koop Awards, The Koop Award Committee is known for its embrace of WTF arithmetic, and it’s that time of year again during which they put their very good brains on full display. For instance, they once gave an award to Pfizer for saving $9 million, or roughly $300 per employee. How did Pfizer do that? With a 2% risk factor decline. Pfizer’s WTF worked out to about 150.
As a sidebar, Pfizer’s award application includes our all-time favorite displays:
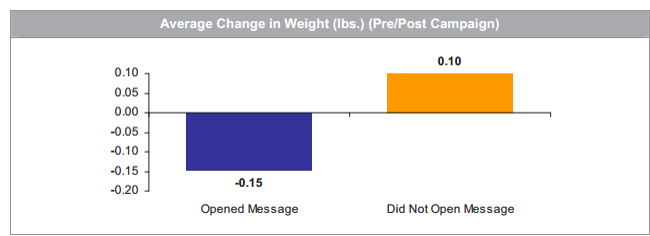
Pfizer’s wellness team sent employees emails on weight control tips. Those who opened the messages lost about 3 ounces while those who did not open the messages gained 2 ounces. That could easily be accounted for by the number of calories required to open the emails.
The 2019 Koop Award
Most recently, the very stable geniuses just gave an award to Baylor Medical School, where, in keeping with tradition, risk factors declined by a whopping 1% — at least among the 25% of the workforce willing to be screened twice (!!!) a year to earn a 20% premium reduction. Let’s take a looksee at the biometric screening results:

On average, these five categories improved 1.04%, to be exact. This is actually quite an accomplishment for the vendor, Vitality, which typically gets no improvement or a deterioration.
The claimed savings — in keeping with Koop Award tradition, buried deep on another page — were $333/year, yielding a WTF of 320.
For any readers out there with the IQs of a Koop Award Committee member, let me spell out the pattern you’re seeing: the wellness industry’s own data yields WTFs 150 to 336 times greater than the wellness industry’s own guidebook estimates.
If anyone would like to reach me to review this arithmetic, or report their own vendor’s results, contact me directly. Schedule-wise, I’m not available today (Monday) or Tuesday. However I am available later this week, specifically WTF.
Share this:


A “cure” for surprise medical billing? Webinar featuring Dr. Marty Makary
Attention, employers with wellness programs: this is bigger than broccoli.

No employee bankruptcy has ever been attributed to a broccoli deficiency. By contrast, surprise medical bills like this one are the #1 source of bankruptcies, wage garnishments and lawsuits against employees. You may have a stress management vendor and a financial wellness vendor, But their programs don’t cover the #1 source of avoidable stress related to financial wellness, for the simple reason that they don’t know how.
The Validation Institute to the rescue.
The Validation Institute is doing a webinar describing an actual cure for employee surprise medical bills for emergency visits and admits. it features the leading experts in pricing and surprise billing, including the bestselling author of The Price We Pay, Dr. Marty Makary. Here is the invitation.

October 31st webinar featuring bestselling author Dr. Marty Makary: A “cure” for employees’ surprise medical bills
You think Halloween is scary? Try surprise medical bills. That’s the subject of this groundbreaking October 31st webinar (register here).
Surprise bills may or may not be the #1 source of workplace stress – but they are certainly the #1 avoidable source of workplace stress. 57% of Americans report receiving one on the last five years. If you have not received complaints from employees about them, or noticed wages being garnished by providers, that’s probably because your health benefit is so generous that you are paying these bills without realizing it…inflating your own costs unnecessarily.
And yet there is a “cure,” at least for surprise bills related to emergency visits and admissions. The Validation Institute and Health Rosetta have assembled what they call the “dream team” of experts in pricing and consent-to-treatment to show you – in a mere hour – how to put the kibosh on this scourge. Presenters include:
- New York Times-bestselling author Dr. Marty Makary, whose blockbuster healthcare exposé, The Price We Pay, has already changed some outrageous hospital billing practices, will describe what consent-to-treatment entails, and why your employees should never just sign the forms thrust in front of them
- Industry pricing gurus Marilyn Bartlett (who saved Montana tens of millions through payment reform) and Health Rosetta-accredited broker-of-the-year Dave Contorno will provide a quick lesson in how to avoid paying inflated charges generally
- Quizzify CEO and trade-bestselling author Al Lewis will then combine these experts’ insights into an elegant one-sentence sticker to add to an insurance card that caps charges and avoids overtreatment…while ensuring employees get the care they need.
Attendees will be able to begin solving the surprise medical bills problem within weeks or even days. If you combine Quizzify’s quizzes with the solution as described in the webinar, it will do to surprise medical bills for emergency care what garlic does to vampires.
Here’s the link to the October 31 webinar registration.
Share this:

“Arithmetically impossible”: Al Lewis talks wellness outcomes with Stacey Richter
The. Numbers. Don’t. Add. Up.
Listen to the Podcast with healthcare guru Stacy Richter to find out why. Here’s what she has to say;
Employers are getting wise to a lot of things right now. I’d suggest a fast follow-on is going to be their view of these wellness programs. It will be interesting to see if current vendors are able to compete with the newer solutions that actually work and which employees actually appreciate. It will also be interesting to see if there’s any backlash against the supply chain that continues to offer up these solutions, especially given some of the lawsuits that are currently under way and all the research which is eminently available.
After about ten people wrote in looking to hear an interview with him, in this health care podcast I’m honored and pleased to speak with the one and only Al Lewis. Al is basically synonymous with wellness programs’ analysis and evaluation. One of my favorite things about Al is that he is as controversial as he is respected. He’s been called both “the founding father” of disease management, and he’s also been called the “troublemaker-in-chief” of the wellness industry. Regardless of your opinion of Al’s views, his integrity and commitment and rigorous analytical approach is open and shut. Al is the author of two books, which you can find in the show notes. He’s also the CEO of Quizzify. Quizzify is a company and an approach that teaches employees how to get the care they need while avoiding the “care” they don’t. Quizzify’s claims have been validated, by the way, by the Validation Institute.
Here’s the link. Happy listening (unless you’re an outcomes-based wellness vendor).
Share this:

Surprise medical bill of the week: $650,000 for a $7000 operation
It’s not about the broccoli, folks.
The major hazard facing employees today is not a broccoli deficiency, but rather: surprise medical bills. And here is one that boggles the mind: $650,000 for a $7000 surgery. Even when these emergencies are “covered” (meaning you pay their bill, except for the four-figure co-insurance), these bills create stress, both emotional and financial, far in excess of stress created by any problem that can be solved by eating more fruits and vegetables. The rate of these bills is also about 100 times the rate of diabetes admissions and heart attacks combined: more than half of Americans report receiving one in the last five years.
Further, people — even people who eat plenty of fruits and vegetables — live in fear of receiving one. Often one such bill can force a family into bankruptcy.
So perhaps it’s time to rejigger your wellness priorities in favor of this most pressing problem? And the other thing is, unlike risk factors (which rarely decline in a population by more than 1-2%, excluding dropouts anyway, according to the Health Enhancement Research Organization), this problem is solvable. Naturally, your wellness vendor has no clue how to solve it, so pay close attention to the following paragraph.
The “long version” of the solution can be found here, But if you don’t feel like clicking through to it, here is the short version: give your employees a sticker to put on their insurance card that says:
“I consent to appropriate treatment and to be responsible for reasonable charges not covered by insurance, up to 2 times the Medicare rate.”
Then you need to educate your employees — using Quizzify or an endless stream of memos, as you prefer — to do two things:
- Carry the insurance card and show the insurance card. It’s not enough to say: “Oh, yeah, I’m covered by so-and-so,” and have the intake person verify eligibility.”
- Do not sign the “terms and conditions” they thrust at you. That boldfaced sentence above contains the consent language needed. They have to treat you, based on that consent.
Unlike attempting to create a more broccoli-centric workplace, this is exactly the type of behavior change you can get widespread acceptance of. Nothing like the threat of bankruptcy to motivate employees to put a sticker on their insurance card.
Share this:


Review of The Price We Pay, by Dr. Marty Makary
Aside from the many antediluvian wellness promoters still insisting that the country’s healthcare cost crisis can be solved by browbeating employees into pretending to eat more broccoli, there is a legitimate debate between:
- those who argue that the system is corrupt because pricing is out of control vs.
- those who argue the system is corrupt because utilization is out of control.
The Price We Pay – certain to be a New York Times bestseller like Dr. Makary’s Unaccountable—shows quite definitively that the answer is both. Our focus in TSW is largely on the wellness industry’s stock-in-trade (I’m looking at you, Interactive Health) — hyperdiagnosis and overtreatment:
“If overtreatment were a disease, it would rank as one of our leading public health threats.”
There is precisely one vendor combating overtreatment at the employee level, of course…and so it’s no surprise that Quizzify gets a nice shout-out. It’s one of only 3 employee health services vendors, out of thousands, mentioned positively. And our work at TSW is recognized too. Here is a brief excerpt of the shout-out:
Al Lewis went from a wellness industry advocate to its foremost critic. He spent years in the industry but came to see its futility. He left and started his own company, Quizzify. The company educates employees about overtreatment and dispels myths about healthy living. I traveled to meet with Lewis, and he didn’t hold back.
“Most of it is fluff. And I might add expensive fluff,” Lewis, a tall man beaming with a smile, explained to me over a snack after he had just finished speaking to a large audience. Quizzify uses an interactive game show approach to teach people about common medical pitfalls, including the risks of overscreening. It also alerts employees to the most common unnecessary tests and procedures in medicine today, according to the Choosing Wisely campaign.
Painstakingly researched with a team of dedicated and highly skilled students and fellows, Dr. Makary traveled around the country collecting first-hand stories at an on-the-ground level rarely seen in health services research.
Dr. Makary has created a niche as a practicing surgeon who also does on-the-ground-research and who also influences health policy. No one else does all three and only few people, like Atul Gawande, do even two of those three. Hence these are not just stories for their own sake, but they feed into the national debate. With the help of this group to raise awareness, they could win the national debate.
One such set of stories, about hospitals suing patients for unpaid bills as a matter of course, has already been featured on NPR, and the hospital in question, Mary Washington in Virginia, has already agreed to cease and desist.
In another city — Carlsbad, New Mexico — it appears that a very significant portion of all the households had been sued by the city’s hospital. This particular chapter reads like fiction. To parse it in detail to the slam-bang climax would require a spoiler alert. Suffice it to say that after you read it, you will want to sell short the corporation that owns the city’s hospital. Except that the corporation in question – notorious among healthcare industry insiders for having made one of the worst acquisitions in hospital industry history earlier in this decade – is already near bankruptcy. The strategy of suing patients is a last-ditch attempt to prevent it. Not much left to short.
Many hospitals sue patients, as we learn in this book. But it’s not just the hospitals. Turns out there are even worse offenders: ambulances. Air ambulances are the worst of the worst, with one example of a bill for an air ambulance ride that exceed the actual bill from the hospital for a one-week stay.
These companies’ strategies are driven by greed rather than need, it would appear, seeking out patients not with the greatest gaps in care or health disparities but with the greatest ability to pay, which explains why 24 air ambulance companies operate in Dallas vs. none in the Medicaid-intensive Rio Grande Valley.
The bottom line is that surprise billing is way worse than I thought…and I thought it was pretty bad. Fortunately, the book recommends some ways to mitigate it.
Inspired by this book, I’ve created a solution, which is that the health insurance card should carry a “battlefield consent” to treatment in the ER and an agreement to be responsible for reasonable charges not to exceed X times Medicare. ERs have to treat you, if you come in. That’s the law. You just don’t have to agree to open-ended charges by signing their preprinted ‘terms and conditions.’ Absent this Battlefield Consent card, you’d either be exposed to open-ended billing or have to negotiate on the spot. Good luck with that. A health insurance card like this would create the equivalent of an advance directive for ER billing.
And what would a thoughtful healthcare policy book be without dissing wellness?
Here’s a shocker: Quite ironically considering that he works at the same institution as Ron Goetzel, Dr. Makary hates “pry, poke and prod” wellness programs. (Johns Hopkins’ excellent wellness program excludes them.) The ‘screening-industrial complex,’ he calls it. Which indeed it is. What, he asks, is so difficult about screening according to USPSTF guidelines — other than depriving wellness vendors of valuable revenues drained from employer coffers? Vendor coaching doesn’t come off much better:
A friend invited me to sit in on a company’s wellness class. I can sum up the instructor’s message in three words: “Avoid fatty foods.” There are a few problems with that message. First, it was about the only thing the health “coach” said to the 20 or so bored people in the room. But second, I cringed because it has absolutely no scientific basis. This class risked making people less healthy; it was loaded with misinformation.
The Price We Pay is already close enough to the top of the Amazon rankings that we can nudge it onto the NYT bestseller list. Every member of TSW Nation should be buying a copy, reviewing it on Amazon, and circulating the reviews loudly on social media.
Share this:

Are Livongo’s outcomes real?
Kudos to employers who have resisted the entreaties of their carriers to jump on the Livongo bandwagon. Resistance is not easy — carriers will pester employers endlessly because they get a nice commission every time an employer bites. As does Mercer, which has a “strategic alliance” with them, but I’m sure they disclose their financial arragement to their employer clients…
Instead, I would simply recommend waiting until Livongo answers these seven questions that they apparently can’t answer. Or they can, but choose not to. Not sure which inspires less confidence.
The references below mention a “study.”, By way of background, this study was conducted by Livongo’s employees, along with employees of its partnered diabetes supply company (Eli Lilly), which also funded the study. So there couldn’t possibly have been any conflict of interest, right? Right?
It was published in something called the Journal of Medical Economics (JME). And no, I hadn’t heard of this publication either. Turns out it’s an “open-access” journal offering “accelerated publication,” where you pay to publish. The Impact Factor is 1.9.
Not familiar with Impact Factors? Those measure the influence of a publication. For instance, the New England Journal of Medicine tallies a 70.8. How hard is it to only get a 1.9? Even the American Journal of Health Promotion (AJHP), which recently proposed charging employees for insurance by the pound, scratches out a 2.6. Possibly, that’s because AJHP does sprinkle more humor into its content than JME, like:
I guess that means 10 states both prohibit it and allow it.
Question #1 for Livongo
Even journals where companies pay to place their articles (need to do a little peer review (which itself is increasingly considered to be a joke), and this peer review was pretty basic: the authors were asked to disclose that the study couldn’t draw any causal relationship between the Livongo intervention and the results. The title of the article itself says that reduced medical spending is “associated with” their product. Later the authors say the results “imply” the product works.
So if the study showed only a correlation and not causation, why does Livongo’s press release announce:
“The findings showed that by using its remote digital health platform, the Livongo for Diabetes program delivered an $88 per member monthly reduction” ?
Question #2 for Livongo
Since these alleged findings are the opposite of Livongo’s initial claim below, featured in a recent Valid Points posting about diabetes vendors snookering purchasers, the second question is, how did the original 59% reduction claim (which basically requires eliminating every hospitalization not connected with births, trauma or cancer) get replaced by the opposite claim that large reductions in physician visits generate all the savings, while admissions increased?

A while back, I actually looked into the likelihood that tighter glycemic control, which itself is rather controversial, (“there is good evidence that intensive control of blood glucose increases patients’ relative risk of severe hypoglycemia by 30%”) could reduce hospitalizations. I used very optimistic assumptions (since I was consulting for a company making a glucometer with remote capabilities, not unlike the one Livongo pitches). Here’s what I came up with: savings of $27 per diabetic per year in inpatient admissions, as opposed to Livongo’s $88 per diabetic per month.
In all fairness to Livongo, they don’t promote that inpatient admissions result anymore (I may have missed the apology for fudging that outcome in the first place), focusing instead on getting doctors paid less money.
Seems curious that physicians would be doing more work – more notifications from remote monitoring devices about blood sugar, more titrating dosages – and be perfectly fine making 26% less money. Plus, every other wellness vendor brags about how many more physician visits they generate, not how many fewer.
Question #3 for Livongo
If I’m seeking a vendor to control diabetes in my population (assuming that is even possible on a broad scale), I would look for weight loss (without which diabetes reversal is basically impossible, but then again sustained weight loss itself is pretty close to impossible) as the leading indicator.
As an intermediate indicator, I would measure units of insulin use across the entire population. That should decline if people are eating much better and exercising much more and losing weight.
The end-point indicator would be a decrease in admissions for diabetes. Of course, since diabetes admissions generally increase following retirement, it isn’t exactly easy to save money in decreased admissions for diabetes, for the simple reason that there hardly are any.
Specifically, for the last year in which a full set is available (2014),158 million commercially insured <65 people generated 126,710 admissions for diabetes. Meaning that in the commercially insured population, the admission rate is so low that a 10% reduction in admissions (which has never been achieved in any population health program) would mean that an employer with 10,000 employees would avoid — get ready — 1 admission.
We suspect Livongo knows this because they listed the diabetes diagnosis codes in their appendix, and it takes about 5 minutes to tally the US admission rate for those codes using the federal database designed for that purpose. And if they don’t know it, they should. Any health services researcher should be aware of this database.
So why didn’t Livongo measure any of those three outcomes? Or did they measure them and decide not to report them?
I’m not sure which answer is “right”: While I would be very concerned if they were suppressing data, I think I would be even more concerned if they didn’t know enough about diabetes to measure the key outcomes.
Question 4 for Livongo
Why did Livongo measure participants against non-participants, when that study design is known to be completely invalid? Benchmarking a par-vs-non-par result has been done five times, including three times by wellness promoters hoping to prove validity of the design The conclusion in each case: 100% of difference in outcomes between the two groups is attributable to the study design, and 0% to the intervention. The design is 100% invalid.
There was actually a case in which the two groups were separated and “match-controlled” in 2004, but the program didn’t start until 2006. During the 2-year period following separation but before the program became available to participate in, the would-be participants nonetheless dramatically outperformed the non-participants…despite not having a program to participate in. (This result caused quite a ruckus in the wellness industry once they realized what they had done.)

Further, more than 15% of the initial Livongo participants dropped out. Assuming dropouts largely failed, aren’t the authors of the Journal article overstating the outcomes for the participant group as a whole by not counting dropouts? Isn’t that like on-time performance statistics not accounting for planes that crashed?
Question 5 for Livongo (really multiple questions)
Livongo offers “free unlimited glucose test strips” to try to reach a “target level of glucose control of Hb A1c <6.5%.”
It is not quite clear that either unlimited free strips or a 6.5% Hb A1c target are good for diabetics. Why, one might ask, does the American College of Physicians propose 7% to 8% instead of 6.5%? While it is true that the American Diabetes Association is sticking with its much lower blood sugar goal, isn’t it also the case that the ADA is largely funded by companies that make products to help lower blood sugar?
And what is the rationale for encouraging more use of glucose strips while Choosing Wisely recommends less testing for many Type 2 diabetics (in JAMA Internal Medicine, impact factor 20)? Exact words:
This recommendation is based on robust evidence, including a Cochrane review of 12 randomized clinical trials with more than 3000 patients, showing no statistical difference between patients who do not self-monitor their blood glucose multiple times per day and those who do self-monitor their blood glucose multiple times per day in glycemic control, nor evidence of effects on health-related quality of life, patient satisfaction, or decreased number of hypoglycemic episodes.
Question 6 for Livongo
Can you explain this passage?
The results also indicate significant reductions in hypercholesterolemia-related spending (2.8%), hypertension-related spending (5.3%), outpatient hospital spending (3.7%), and utilization in outpatient hospitals (1.3%) and office visits (5.6%).
Specifically, is there any literature whatsoever that says doing more blood sugar checks reduces spending on cholesterol and blood pressure drugs? Were you just “shopping” for retrospective correlations?
Why would “outpatient hospitals” decline? What do ambulatory surgery centers have to do with checking your blood sugar?
Question 7 for Livongo
Why are your Amazon and BBB reviews so bad?
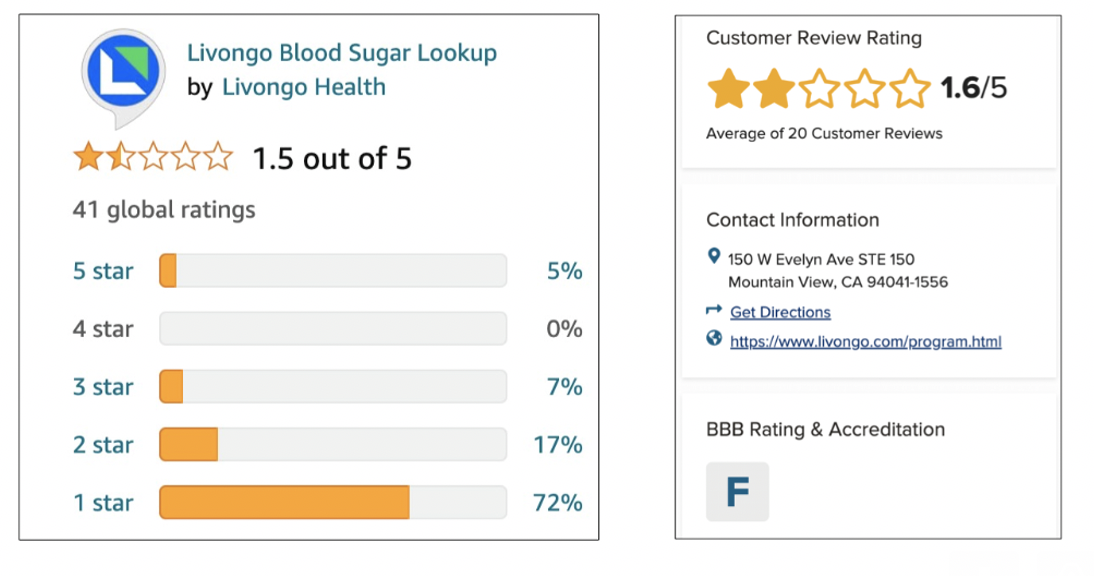
One of the reviewers claims that a Livongo “tip” is: “Did you know that not getting enough sleep can make you cranky and out of sorts?” Is this true?
So it could be that this is just me, since their revenues are doubling every year. Maybe, like in the rest of wellness, answering questions about efficacy is beside the point. Maybe the point in HR is just to do something, regardless of whether it works, in case someone in the C-Suite asks. Or in the immortal words of the great philosopher Yogi Berra: “We don’t know where we’re going, but we’re making good time.”
Share this:


Best healthcare joke ever
You rarely see the words “healthcare” and “joke” together — except of course figuratively, when we’re talking about certain wellness vendors. And we have never put an actual joke on this blog. However, this one is too good to pass up — and is also exactly what’s wrong with our healthcare system, that Quizzify addresses. [SPOILER ALERT: It’s also a “soft” PG, in case anyone might be offended. To put this in perspective, these wellness vendors are much more offensive…and yet they’re rated G.]

A guy has had these splitting headaches for years. Tried everything but they won’t go away, so he goes to the doctor for a battery of tests. He happily signs up for all of them, because he is fully covered — and he really, really, wants to get rid of these splitting headaches.
The results come back. The doctor says: “According to our tests, there is nothing we can do for you except to remove your testicles. So think it over.”
The guy thinks it over for a few days — two really bad options, but finally decides that getting rid of the headaches is more important. Gets the operation and lo and behold, the pain is gone immediately.
On the way home, he is so happy with his new, pain-free life, that, passing a tailor along the way, he decides to treat himself to a new suit. He goes in, tells the tailor he wants a new suit. The tailor, who’s about 75 years old, looks the guy up and down and says: “42 Long.”
The guy says: “Yes, how’d you know?”
The tailor replies: “I’ve been in this business 55 years. I know all this stuff.”
The guy says: “While I’m at it, I guess I should get a new shirt to go with the suit.”
The tailor looks at him again and says: “Sure. 16 1/2 -34?”
The guy says: “Right again. How’d you know?”
The tailor says: “I’ve been in this business 55 years. I know everything there is to know about fitting men’s clothes.”
The guy gets the suit and the shirt, and then, as he is about to leave, says: “You know, while I’m here, I might as well get some new underwear.”
The tailor looks at him and says: “Sure. 38, right?”
The guy says: “You’re wrong this time. 36.”
The tailor says: “No, you’re definitely a 38.”
The guy says: “Nope. I wear 36.”
The tailor says: “Trust me. You’re a 38. Underwear that’s too tight will squeeze your balls together. You’ll get these splitting headaches.”

